Osteochondroma of the Distal Fibula causing Disruption of the Syndesmosis


Clinical History
A 21-year-old female presented with a sprained ankle with no history of trauma.
Imaging Findings
This 21-year-old lady presented to the emergency department of a large teaching hospital after sustaining an inversion injury to her right ankle, resulting in a “sprain”. She had no previous problems with her ankle and no past medical history of note. Examination of the limb revealed soft-tissue swelling medially and tenderness over the medial joint line with reduced range of movement at the ankle joint.
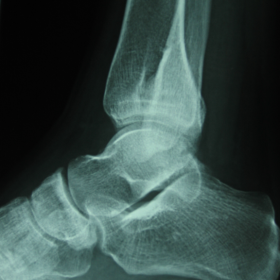
Plain radiographs were performed and appearances were consistent with an osteochondroma of the distal fibula that was causing disruption to the syndesmosis, with a fracture through the articular surface of the tibia.
This patient was treated conservatively as the cause of her symptoms was a “sprain” to the ankle, the findings of an osteo-chondroma being incidental in this case. At follow-up two weeks later her pain was resolving and she was discharged.
Discussion
The WHO definition of an osteochondroma is a cartilage-capped bony projection arising from the external surface of the bone containing a marrow cavity that is continuous with that of the underlying bone. They may occur as solitary or multiple lesions, and can form at any time from birth until the cessation of bony growth. Macroscopically, lesions are divided in to pedunculated where there is a visible ‘stalk’, or sessile if this is absent. The incidence of bone tumours in european populations being quoted at 79 per 1 million of population [1], and osteochondroma is the most common benign bone tumour, accounting for more than a third [2], although the true incidence may be higher in view of the asymptomatic nature of some lesions. Herediatry Multiple Exostosis, a genetically heterogenous autosomal dominant condition, is characterised by the growth of more than two osteochondromas and having a male preponderance with a ratio of 3:2. This condition is associated with a risk of progression to the formation of chondrosarcoma, quoted at 0.5-5% [3].
The commonest sites for osteochondroma growth are distal femur [4], proximal tibia and the intra-articular surface of the knee. However they have also been known to affect the mandible [5], scapula, pelvis, distal tibia,fibula radius and hand [6,7]. Lesions involving the spine can be associated with spinal cord compression although this is a rare location for tumour growth [8]. The literature reports an extreme case where osteochondroma in a patient with hereditary multiple exostosis lead to diaphragmatic rupture and bowel obstruction requiring surgical intervention [9].
Symptoms range from pain, loss of movement, swelling, cosmetic dysfunction and fracture following low energy trauma. Symptoms may also manifest as a result of direct pressure from the exostosis on surrounding neurovascular structures and incidences of acute lower limb ischemia secondary to fracture of osteochondroma have been described [10]. The growing lesions have also been described to grow through the mid-substance of peroneal nerve [11].
Surgical excision of symptomatic solitary osteochondromas has been demonstrated to have a low severe complication rate (<5%), with a high percentage (93%) of preoperative symptoms resolving [12]. Long term follow up of surgical interventions in solitary lesions shows favourable results with recurrence rates quoted at 18% and further oncognesis quoted at <2% [13].
Solitary Osteochondromas affecting the distal tibia are often more symptomatic than those affecting distal fibula. In patients with open growth plates and a large tumour causing local symptoms, partial excision preserving the physis may be beneficial in terms of symptom relief [14].
Treatment of solitary osteochondromata presenting with fractures remains uncertain and undefined, although of those who engage in sports, surgical excision could be preferential as it allows return to sporting activity sooner than those managed non-surgically [15].
MR imaging can be of use in the follow-up of these patients to detect any malignant transformation. MR is the most accurate method of measuring cartilage cap thickness which is an important criterion for differentiating between osteochondromas and low-grade osteosarcomas [16].
Differential Diagnosis List
Final Diagnosis
Distal Fibular Osteochondroma with Syndesmosis Disruption
Liscense
Figures
X-rays of the distal tibia and fibula


Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided ankle X-ray, there is a localized bony protrusion at the distal tibia (near the articular surface). It appears continuous with the cortex, showing outward bone projection, likely covered by cartilage on its surface. No obvious signs of soft tissue swelling are observed. The joint space is acceptable, with no apparent fracture line or acute traumatic findings. Overall, there is no distinct bone destruction or notable soft tissue mass visible on the images.
II. Possible Diagnoses
- Osteochondroma: One of the most common benign bone tumors. It is typically characterized by a bony outgrowth continuous with the bone marrow cavity, covered by a cartilaginous cap. The patient’s young age, lack of significant trauma history, and the presence of an ankle protrusion are consistent with the usual clinical and imaging features of osteochondroma.
- Chondrosarcoma: Generally considered when there is a long-term history, thickening of the cartilaginous cap, or malignant changes in the lesion. In this case, the patient is quite young, and the X-ray does not show any obvious invasive lesions or soft tissue swelling. If clinical symptoms are not severe, the likelihood is quite low and more of a differential diagnosis consideration.
- Other benign bony prominences or bone spurs: Such as osteophytes, which typically affect the articular surface or margin. Further evaluation of the specific location and symptomatology is needed to distinguish these.
III. Final Diagnosis
Taking into account the patient’s age, imaging characteristics, and clinical presentation, the most likely diagnosis is:
Solitary Osteochondroma.
If clinical symptoms worsen, the protrusion grows rapidly, or there is abnormal thickening of the cartilaginous cap, further imaging evaluations (e.g., MRI) or pathological examination may be required to rule out rare malignant transformation.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Conservative Treatment: For solitary osteochondromas with no significant or only mild symptoms that do not affect joint function or daily life, observation and follow-up can be chosen. If needed, periodic imaging (X-ray or MRI) is recommended to monitor lesion size and cartilaginous cap thickness.
- Surgical Treatment: If there are prominent symptoms (pain, limited activity, nerve or vascular compression, etc.) or if suspicious changes are noted, surgical resection is recommended. Surgery can effectively remove the tumor and relieve pain, with relatively low rates of postoperative complications and generally favorable prognosis.
2. Rehabilitation and Exercise Prescription
During postoperative care or conservative treatment, individualized rehabilitation exercises and an exercise prescription should be developed based on the function of the ankle joint and the location of the osteochondroma, following the FITT-VP principle (Frequency, Intensity, Time, Type, Progression, Volume & Progression).
- Early Recovery Phase: Focus on protective activities, avoiding excessive weight-bearing or intense twisting of the ankle. Include joint range-of-motion exercises, such as ankle circles, toe gripping, and isometric exercises for foot muscles to promote blood circulation and reduce swelling.
- Intermediate Strengthening: Gradually increase weight-bearing exercises, such as straight-line walking and resistance training with elastic bands. Maintain joint stability and strengthen specific muscle groups, including the triceps surae and tibialis anterior.
- Advanced Phase: When pain and function allow, add balance training (balance boards or single-leg standing) and progressively introduce light jumping and jogging. Monitor the ankle’s response, and adjust intensity if discomfort occurs.
- Training Frequency and Intensity: Conduct exercises 3-5 times per week, 15-30 minutes each session, focusing on joint mobility and muscle strength. Begin with low to moderate intensity, gradually progressing to moderate intensity.
- Follow-Up and Adjustments: Regular follow-up is recommended. Based on symptom changes and imaging findings, evaluate whether further intervention or modifications to the rehabilitation plan are necessary.
Note: If you experience significant pain, swelling, or any discomfort during rehabilitation, suspend the exercises immediately and consult a professional.
Disclaimer
This report is only a reference based on the provided medical history and imaging data. It cannot replace an in-person consultation or a professional doctor’s opinion. If you have any questions or if symptoms worsen, please seek specialist medical advice promptly.
Human Doctor Final Diagnosis
Distal Fibular Osteochondroma with Syndesmosis Disruption