A postraumatic lesion of the pelvis



Clinical History
A 14 year old boy suffered from severe pain in the left hip region after school sports. The definite diagnosis was made by MRI and a conservative therapy was initiated.
Imaging Findings
A 14 year old boy developed severe pain above the left hip during school sports when playing soccer. Physical examination revealed a localised pain in the left inguinal area with a painfull tenderness. Flexion of the hip was painfully reduced. Radiography of the pelvis revealed a prominent anterior inferior iliac spine. A MRI of the hip on a 1.0T Siemens Harmony scanner was performed and an avulsion fracture of the apophysis of the anterior inferior iliac spine was diagnosed. Therapy strategy remained conservative with bed rest and analgesia and stepwise mobilization.
Discussion
Pelvic apophyseal fractures typically affect adolescents after a sudden contraction of a muscle to the immature musculo-skeleton junction [1]. Avulsion fractures of the pelvis were found in approximately 16% of pelvic injuries that required a pelvic x-ray [2]. Among these lesions those of the anterior inferior iliac spine have been described as second frequently avulsion fractures (21,5%). The injury mechanism is a combination of a sudden hip hyperextension and knee flexion leading to maximum stress on the physis at the attachment of the rectus femoris muscle. This is the weakest part of this osseotendinous junction in young adults. These movements are observed by kicking a ball (soccer), jumping over hurdles and gymnastics [1, 2].
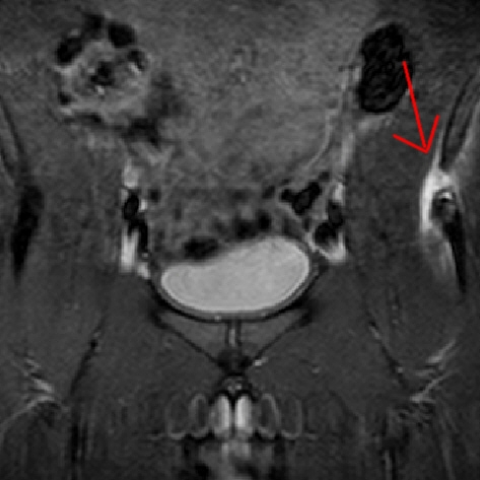
Diagnosis of theses lesions is made by ultrasound, CT or MRI while X-ray is usually without pathological findings [3]. X-ray in our case did not reveal any osseous lesion except from a slight prominence of the left anterior inferior iliac spine (Fig. 1, 2) while T2 weighted and T1 weigted fat saturated MRI sequences revealed fluid surrounding and osseous oedema within this structure (Fig. 3, 4) as well as the distracted osseous fragment (Fig. 5).
Sonographically widening of the physis or slight displacement of the apophysis in comparison to the contralateral side with oedema or hemorrhage indicate an avulsion fracture [4]. CT usually proves the alvusion fragment while hematoma and oedema are striking on MRI images [3, 4].
Treatment is generally conservative. Sufficient analgesia and bed rest are administered in the acute stage followed by stepwise mobilization afterwards for 3 weeks to 4 months until full function and painlessness is reached [1, 3, 5]. If a severe distraction of the fracture is diagnosed or conservative management fails surgical reattachment of the dislocated fragment is the method of choice [5].
Differential Diagnosis List
Final Diagnosis
Left sided pelvic apophyseal fracture.
Liscense
Figures
Axial X-ray of the left hip

X-ray of pelvis

Tirm cor
T2TSE sag

T1 GRE Fatsat

Imaging Findings
Based on the provided imaging data of the Anterior Inferior Iliac Spine (AIIS) region, the following main features can be observed:
- Conventional X-ray examination: No obvious fracture line is visible, only a slight prominence on the left anterior inferior iliac spine.
- MRI findings: On T2-weighted and fat-suppressed T1-weighted sequences, there is marked edema and fluid signal at the left AIIS. A small bony avulsion fragment is present, separated from the structure at the tendon attachment site.
- Overall presentation: Suggestive of an avulsion fracture at the tendon attachment site, accompanied by local soft tissue edema or possible hemorrhage.
Potential Diagnoses
- Avulsion Fracture (Anterior Inferior Iliac Spine)
Occurs due to sudden, forceful muscle contraction (such as kicking a ball, jumping, etc.) acting on an incompletely matured epiphysis or bony prominence, frequently leading to tendon attachment avulsion. - Soft Tissue Strain or Tendon Attachment Injury
If the bone is intact, local soft tissue edema could indicate muscle or tendon injury. However, the presence of a small bony fragment on MRI makes this less likely. - Stress Fracture
Repeated stress can theoretically lead to a stress fracture at an epiphysis or bony prominence, but the imaging findings usually differ from those of an avulsion fracture.
Final Diagnosis
Considering the patient's age, type of physical activity (e.g., playing soccer or hurdling), clinical presentation (acute hip pain), and MRI findings (bony avulsion fragment and surrounding edema), the most likely diagnosis is:
Left Anterior Inferior Iliac Spine Avulsion Fracture
Treatment Plan and Rehabilitation Program
Once an avulsion fracture is confirmed, the treatment approach depends on the degree of fragment displacement and symptom severity:
- Conservative Treatment
- During the acute phase, limit weight-bearing and activities. Bed rest for 1–2 weeks may be necessary.
- Provide adequate pain control to prevent protective postures and further injury resulting from pain.
- Follow-up imaging reviews should guide the gradual increase in activity levels based on pain and fracture healing progress.
- Surgical Treatment
If the avulsed bony fragment is significantly displaced or if severe pain and functional limitation persist after conservative treatment, surgical reduction and fixation may be considered.
After initial treatment, an individualized rehabilitation plan should be developed, aiming to facilitate fracture healing, restore hip and lower limb strength, and prevent re-injury.
Rehabilitation/Exercise Prescription Recommendations:
- Phase 1 (Acute Phase, 0–2 Weeks)
- Emphasize protective rest and engage in only mild range-of-motion exercises (passive or active light movement without weight-bearing).
- Elevate the affected limb or apply ice packs to reduce pain and swelling.
- Phase 2 (Recovery Phase, 2–6 Weeks)
- Gradually increase small-range joint activities within the pain threshold, such as passive hip flexion and extension exercises in a seated or supine position.
- Begin non-weight-bearing or low-weight-bearing exercises (e.g., wall-supported partial squats, seated isometric contractions) to progressively rebuild core muscle strength.
- Phase 3 (Functional Reinforcement Phase, 6 Weeks and Beyond)
- Gradually incorporate weight-bearing exercises and lower-limb strength training, such as seated or standing ankle-loading drills, or resistance band workouts.
- Resume running, jumping, and other sports-specific drills under professional guidance, keeping a close watch for any pain or discomfort.
Throughout the rehabilitation process, refer to the FITT-VP principle (Frequency, Intensity, Time, Type, Volume, Progression, and Individualization). Adjust the plan based on the patient's reported pain, functional progress, and follow-up imaging findings.
Disclaimer
This report is based on the provided clinical history and imaging data and is intended to offer reference information for diagnosis and treatment. It does not replace a formal in-person consultation or the final medical opinion of a qualified physician.
Human Doctor Final Diagnosis
Left sided pelvic apophyseal fracture.