Primary sternal Ewing’s sarcoma with lung and adrenal metastasis



Clinical History
A thirteen-year-old boy presented with progressive painful swelling over the centre of the chest for 3 months. His vitals were stable on presentation at the hospital. Examination confirmed a firm tender swelling over anterior chest covering the sternum. A chest radiograph followed by a contrast-enhanced CT of the chest and upper abdomen was done.
Imaging Findings
The Chest radiograph (PA view) demonstrated an ill-defined central mass occupying the mediastinum with poorly maintained margins with the mediastinal vascular structures and cardiac silhouette. Multiple well-defined rounded opacities were noted in bilateral lung fields. Right-sided pleural effusion was also present (Figure 1).
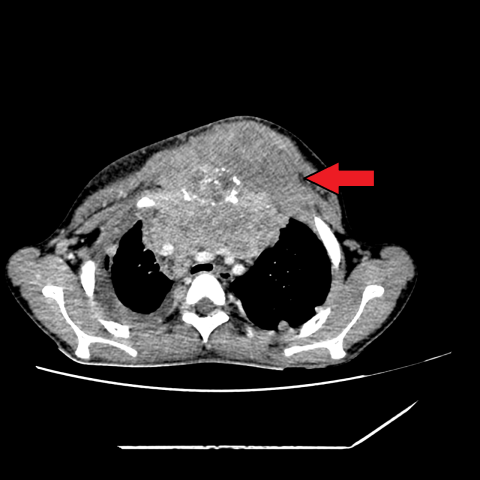
Imaging by CECT revealed a large ill-defined heterogeneously enhancing soft tissue lesion which demonstrated permeative destructive pattern within the manubrium and upper half of the sternum, extending into the anterior mediastinum and loss of fat plane with adjacent chest wall muscles (Figure 2). Multiple widespread lung nodules and right-sided pleural effusion were noted (Figure 3).
A large ill-defined heterogeneously enhancing right adrenal mass was detected (Figure 4).
Based on the imaging findings, a provisional diagnosis of Ewing’s sarcoma with lung and adrenal metastasis was made.
Discussion
Background
10-15% of all primary bone tumours are Ewing's sarcomas, the second most frequent malignant bone tumour in adolescents and young adults. Although Ewing's sarcoma can affect any bone, the lower extremity (45%), pelvis (20%), upper extremity (13%), axial skeleton and ribs (13%), and face (2%) are the most prevalent places. The femur is the most frequently affected bone, with the tumour usually arising in the midshaft [4]. 10-15% of all primary chest wall tumours are Ewing sarcomas [5].
Imaging Perspective
When Ewing's sarcoma is detected on a CT scan, the mass is often big, poorly defined, and appears inhomogeneous due to widespread cystic degeneration. Calcification may or may not be present. Smaller tumours tend to be more homogeneous, but larger tumours manifest as heterogeneous masses that commonly show signs of haemorrhage or necrosis [6]. Despite being aggressive, these tumours frequently displace nearby structures at first. However, direct infiltration can destroy ribs and is more common in bigger tumours [5]. Primary adrenal cancer is less common than adrenal metastases. Sarcoma-related metastases to the adrenal glands are uncommon and typically accompany large metastases that affect numerous organs at once [7].
Rhabdomyosarcoma are the most common soft tissue tumour in children. They are usually located in the orbits, but approximately 7% are found in the trunk and thorax. The appearance of the mass is non-specific and indistinguishable from other sarcomas; however, adjacent bone destruction is seen in over 20% of cases [5].
Outcome
One of the most potent indicators of a poor prognosis is the presence of disseminated illness, which can be identified through imaging, cytological testing, and histological analysis of the bone marrow at the time of diagnosis in ESFT [3]. A surgical resection and neoadjuvant chemotherapy and radiotherapy are used as treatments. Long-term survival is possible for people whose tumour is contained to the chest. Overall 5-year survival is between 15-48% [8].
The patient then underwent ultrasound-guided biopsy of the mass. Light microscopy showed multiple small round blue cells with a high nucleo:cytoplasmic ratio arranged in sheets and clusters (Figure 5). On Immunohistochemistry (IHC), the tumour cells were positive for CD99 and negative for K, LCA, Synaptophysin, Desmin and Myogenin. The pathology report favoured Ewing's sarcoma.
Being metastatic on presentation, the patient was started on combination chemotherapy.
Written informed patient and parents’ consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Primary sternal Ewing’s sarcoma with lung and adrenal metastasis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures







Medical Analysis Report
I. Imaging Findings
1. The chest X-ray reveals a soft tissue mass in front of the sternum, with unclear boundaries and heterogeneous density, showing local bulging and invasion of the anterior sternal wall.
2. Contrast-enhanced chest CT scan shows a significant soft tissue mass in the anterior chest wall with heterogeneous enhancement, with visible necrotic or cystic areas. The overall boundary is not well-defined, and there are signs of local invasion of the sternum.
3. Scattered possible nodular changes are visible in the lung fields, suggesting lung metastatic nodules.
4. CT at the upper level of the abdomen demonstrates an abnormally enhancing lesion in the right adrenal region, suggesting a possible metastasis.
5. Pathological slides under the light microscope show a small round blue cell tumor featuring deeply stained nuclei and scant cytoplasm, consistent with the characteristics of a small round cell tumor. Immunohistochemistry is positive for CD99, supporting a diagnosis of Ewing sarcoma.
II. Possible Diagnoses
- Ewing Sarcoma (Primary Consideration): Common in adolescents and may involve bones or the chest wall soft tissues. Imaging typically reveals a large, heterogeneous mass. Histologically, it presents as a classic small round blue cell tumor, and CD99 is positive.
- Rhabdomyosarcoma: A common soft tissue sarcoma in children. Its imaging appearance may be similar to other sarcomas, but immunohistochemistry typically shows Desmin and Myogenin positivity. These markers are negative in this case, making rhabdomyosarcoma less likely.
- Other Malignant Chest Wall Tumors (e.g., osteosarcoma, metastatic tumors, etc.): These may lead to sternal destruction or soft tissue masses. However, based on pathology, immunohistochemistry, patient age, and the specificity of CD99, Ewing sarcoma aligns more closely with both the clinical presentation and pathological findings.
III. Final Diagnosis
Considering the patient is a 13-year-old adolescent with a progressively painful mass in the anterior sternal region, imaging findings of local sternal destruction with involvement of surrounding soft tissue, and pathological findings consistent with a small round blue cell tumor that is CD99 positive, alternative differential diagnoses were ruled out. The definitive diagnosis is Ewing sarcoma. Further evaluations indicate metastatic lesions in the adrenal gland and possibly other sites, confirming a diagnosis of Ewing sarcoma with metastases.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Chemotherapy: Chemotherapy is the foundation of treatment for Ewing sarcoma, typically involving combination regimens (e.g., doxorubicin, vincristine, ifosfamide).
- Local Treatment (Surgery and Radiotherapy): For sternal and chest wall involvement, surgical resection can be considered after chemotherapy-induced tumor shrinkage. Radiotherapy may help control the local lesion or parts that cannot be completely resected.
- Treatment of Metastatic Lesions: For confirmed metastatic sites such as the adrenal gland or lung lesions, evaluate the overall condition and response to therapy to determine the best approach, which may include localized radiotherapy or further systemic treatment.
2. Rehabilitation and Exercise Prescription
Given that the patient is currently undergoing intensive cancer treatment, there may be significant fluctuations in physical condition. Rehabilitation and exercise should follow a gradual, individualized principle to ensure safety:
-
Initial Phase (During Chemotherapy):
- Focus on conservative exercises, such as mild bedside or seated activities, including range-of-motion exercises and gentle breathing exercises.
- Each session lasts about 5 to 10 minutes with low intensity. Monitor heart rate and blood pressure to avoid excessive fatigue.
-
Progressive Phase (After Symptom Relief):
- Increase the time spent out of bed. Light indoor walking or brief slow walks downstairs may be introduced, lasting approximately 15 to 20 minutes per session, adjusted according to endurance.
- Pay attention to bone integrity, especially around the sternum, to prevent undue pressure.
-
Consolidation Phase (Late Treatment and Rehabilitation Clinic):
- If the lesion remains stable, low-intensity aerobic exercise such as brisk walking or stationary cycling may be gradually introduced under expert guidance.
- Exercise frequency is recommended at 3 to 5 times per week, maintaining an intensity of “subjectively light to moderate” for about 20 to 30 minutes each session.
- Monitor cardiopulmonary function, blood counts, and other indicators. If there are any abnormalities or significant fatigue, stop exercising and consult a physician promptly.
-
Muscle Strength and Flexibility Training:
- After adapting to basic endurance exercises, gradually incorporate light resistance training and joint stretching. Avoid high-load exercises for the sternum and ribs.
- Discontinue training and seek medical attention if pain worsens or if discomfort around the sternum arises.
Throughout the rehabilitation process, regular follow-up visits and imaging studies are necessary to evaluate tumor control and bone strength. Any exercise plan should be conducted under the supervision of the attending physician and professional rehabilitation therapists.
Disclaimer
This report is a reference-based medical analysis derived from the available imaging and clinical information, aimed at offering professional opinions but cannot replace in-person consultations or the diagnosis and treatment advice of a licensed physician. The specific treatment and rehabilitation plan must be tailored to the individual patient, as determined or adjusted by specialists after comprehensive evaluation.
Human Doctor Final Diagnosis
Primary sternal Ewing’s sarcoma with lung and adrenal metastasis