Soft tissue chondroma of the ulnar wrist



Clinical History
A 73 year old man complained of ulnar wrist pain. A palpable mass was present in his left ulnar wrist, which had been known to him for years, but used to be painless until a week ago.
Imaging Findings
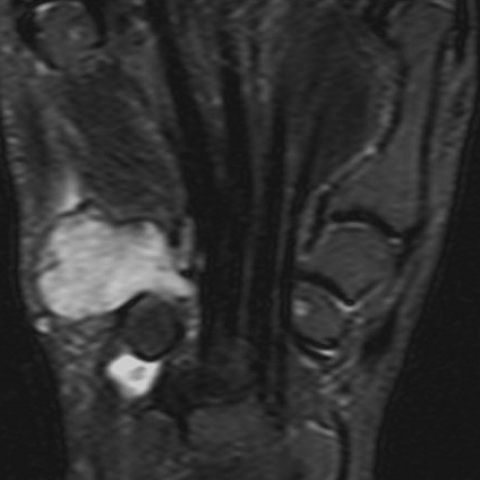
A 73 year old man was referred for imaging studies of the left hand and wrist. He complained of a mass in his ulnar wrist, which had been present for many years, but had become increasingly painful for about a week. The clinical examination confirmed a firm mass situated deep to the hypothenar musculature and extending to the dorsum manus. Dorsal extension of the wrist joint was slightly restricted. Apart from that, the patient’s past history was unremarkable. Plain radiographs of the left hand were obtained. The posteroanterior view showed a soft tissue mass which eroded the ulnar wrist bones and metacarpal bases (Fig 1). MRI better depicted the tumour extent amongst the wrist and metacarpal bones (Fig 2). The lesion completely surrounded the extensor carpi ulnaris tendon, but did not destroy it. On transverse sections, the tendon was situated near the centre of the mass, suggesting that it might have originated from the tendon sheath (Fig. 3). Based on the imaging findings, open excisional biopsy was performed and the specimen was sent to a national reference centre for soft tissue neoplasms, where the diagnosis of a benign, extraskeletal chondroma was made.
Discussion
The vast majority of hand and wrist masses are benign, and many of these have a distinctive appearance on imaging studies, especially MRI. The 3 most common hand and wrist lesions are ganglion cysts, giant cell tumours of the tendon sheath, and haemangiomas [1]. Other common lesions that can be diagnosed radiologically are lipomas, neural sheath tumours, and variant soft-tissue or bony structures [2]. Soft tissue chondromas of the wrist are quite rare. They are also particularly remarkable insofar as they do not arise in the expected location of a chondroma, exhibit similar signal characteristics to enchondromas on MRI (including possible calcifications), and may lead to cortical destructions, making them indistinguishable from malignancies [3]. Typical chondromas in adults arise from nests of chondrocytes within the meta- or diaphyseal bones (enchondroma) or in the periosteum (periostal chondroma). Soft tissue chondromas, on the other hand, are solitary, slowly-growing lesions, mostly involving the tendon sheaths of the hands or feet. However, they are benign neoplasms consisting of mature hyaline cartilage. As in their skeletal counterparts, large tumours may lead to cortical bone destructions, which may become painful. The pathologic features of this tumour type are variable. Focal fibrosis, calcification, ossification, or myxoid changes may occur [4]. Calcifications have been described in most previous reported cases [3]. This case is rather unusual, because there were no intralesional calcifications. On MRI, long T1 and T2 relaxation times in conjunction with a sharply marginated, lobular appearance are consistent with a cartilaginous lesion [3]. In masses of the wrist, less advanced than this one, familiarity with the features of extraskeletal chondroma may be of practical importance to avoid an overly aggressive treatment. However, given the extensive bony erosions of the present tumour, malignant degeneration had to be suspected in spite of the rather long history. Contrast was not administered in this case, but could have been useful to demonstrate an enhancement pattern typical for cartilaginous tumours. However, the lesion had to be biopsied at any rate.
Differential Diagnosis List
Final Diagnosis
Soft tissue chondroma of the wrist
Liscense
Figures
Dorsopalmar DR view

Coronal MRI

Transverse MRI


Imaging Analysis Report
I. Imaging Findings
1. Plain radiographs (X-ray) reveal: A soft tissue mass shadow on the ulnar side of the left wrist. Mild bone erosion or marginal bone changes are seen on the adjacent ulnar carpal surface, with relatively well-defined lesion contours.
2. MRI findings: On T1-weighted images, the lesion’s signal intensity is slightly higher or isointense compared to surrounding soft tissues; on T2-weighted images, it shows high signal intensity with clear, lobulated margins. No obvious calcification signals are observed within the lesion. No apparent bone marrow involvement is seen, and the lesion is mainly confined to the soft tissue, presumably originating from the tendon sheath or near the joint capsule.
3. Lesion morphology: The mass appears relatively regular in shape with clear peripheral boundaries, demonstrating both cystic and solid components, strongly suggestive of cartilaginous features. Local bone shows signs of compression, erosion, or superficial bone destruction.
II. Potential Diagnoses
Based on the patient’s longstanding history without obvious pain until recently intensified pain, as well as the cartilaginous signal characteristics on imaging, the following are considered:
- Soft Tissue Chondroma of the Wrist (suspected exochondroma): Also known as soft tissue chondroma or chondroma of the tendon sheath. It is typically a slowly growing benign cartilaginous tumor. On MRI, it often shows high T2 signal and may present calcification or bone compression changes.
- Giant Cell Tumor of the Tendon Sheath: Commonly found in the fingers or wrist, typically exhibiting isointense or slightly low signal on T1 and low to isointense signal on T2. However, these tumors often show varying degrees of hemosiderin deposition on MRI and usually lack cartilaginous structures.
- Synovial Cyst (Ganglion Cyst) of the Wrist: Most common in this region, generally presenting as a cystic high T2 signal on MRI, without distinct cartilaginous or bone erosion features.
- Chondrosarcoma: In older patients, if there is substantial bone erosion or a sizable soft tissue mass with poorly defined margins, one should be wary of a malignant cartilaginous tumor. However, given this patient’s long-standing history and relatively well-defined margins, a benign lesion is more likely.
III. Final Diagnosis
Considering the 73-year-old male patient, the long-standing mass on the ulnar side of the left wrist, recent exacerbation of pain, and the imaging demonstrations of classic cartilaginous signals with superficial bone erosion, the most likely diagnosis is:
“Soft Tissue Chondroma of the Wrist (Soft Tissue Chondroma / Tendon Sheath Chondroma)”.
Because the lesion is relatively large and exhibits bone changes, a pathological biopsy or surgical exploration is still recommended to further rule out the rare possibility of malignant transformation.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy:
- Surgical Treatment: For lesions of larger size with bone erosion or those causing significant recent symptoms, complete resection, or resection following pathological biopsy, is a common approach.
- Conservative Treatment: If the patient’s symptoms are mild and pathology confirms a benign lesion, regular follow-up may be considered. However, given the patient’s increased pain and bone involvement, the suitability of conservative management may be limited.
- Postoperative Follow-up: Regular imaging follow-up is advised to monitor for recurrence or residual lesions.
2. Rehabilitation/Exercise Prescription:
If surgical treatment is performed, a gradual rehabilitation regime is recommended as follows:
- Acute Phase (1–2 weeks post-surgery): Focus on protecting surgical wounds on the wrist and performing basic active and passive range-of-motion (ROM) exercises for the wrist and fingers. Practice 2–3 times daily, each session lasting 5–10 minutes, ensuring suitable range without significant pain.
- Recovery Phase (2–6 weeks post-surgery): Gradually increase wrist joint range of motion and incorporate mild resistance training (e.g., grip exercises, resistance bands). Follow a “low-intensity, high-frequency” principle, 2–3 sets daily, 10–15 repetitions per set, and progressively increase resistance based on patient tolerance.
- Enhancement Phase (6 weeks or longer post-surgery): Once basic mobility is restored and no significant pain is present, proceed with strengthening and flexibility exercises for the wrist, such as using light dumbbells or targeted wrist extension/flexion exercises. Increase training volume by 5–10% weekly, ensuring no swelling or pain occurs.
- Individualized Monitoring: For older patients or those with other chronic conditions, pay special attention to cardiopulmonary function and bone health. Gradually increase exercise volume and closely monitor the lesion site’s response.
Throughout rehabilitation, consider the FITT-VP principle (Frequency, Intensity, Time, Type, Volume, and Progression). If persistent pain, swelling, or functional limitations arise, prompt reevaluation and adjustment of the plan are necessary.
V. Disclaimer
This report is a reference analysis based on existing imaging and clinical information. It does not replace an in-person consultation or professional medical advice. Final diagnosis and treatment decisions should be made through pathological examination, comprehensive assessment of the patient’s condition, and multidisciplinary consultation.
Human Doctor Final Diagnosis
Soft tissue chondroma of the wrist