Subperiosteal osteoid osteoma in the talar neck



Clinical History
An 18-year-old man presented with a nocturnal pain of the left ankle.
Imaging Findings
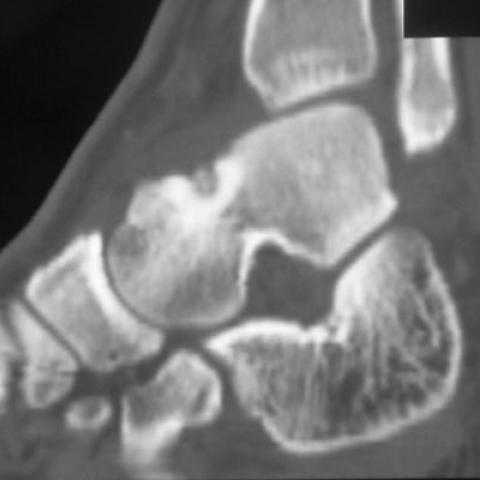
The patient had been enduring a debilitating nocturnal pain of the left ankle for the past four months, and had obtained no relief from steroidal anti-inflammatory drugs. A clinical examination was done, which showed tumefaction of the ankle with limited mobility. A conventional radiography analysis showed a solitary rounded lytic zone, which had geographical contours, and a narrow transitional zone with the healthy bone (Fig. 1). The ultrasonography examination found the presence of intra-articular fluid associated with synovial thickening (Fig. 2). We then suspected a tumoral or a synovial process. The MRI studies showed the presence of a subperiosteal lesion in the talar neck, which had a decreased signal intensity on T1, moderately increased signal on T2, surrounded by a marginal osteosclerosis with decreased intensity on the different sequences, and associated with a central gadolinium- enhancement (Fig. 3). A CT scan showed the presence of a subperiosteal lytic lesion with a partially calcified central nidus surrounded by a marginal osteosclerosis (Fig. 4). The patient underwent surgical excision.
Discussion
Osteoid osteoma is a benign osteogenic tumour that occurs in the young adult. Its localization on short and flat bones is rare. A juxta-articular osteoid osteoma arising around the ankle is unusual (1). Tumors arising on the neck of the talus will commonly produce symptoms mimicking monoarticular arthritis or trauma (1). In the diagnosis of an osteoid osteoma, a history of the relief of pain with the use of aspirin is an important consideration. Plain radiographs are useful. Fine-cut computed tomography scanning or magnetic resonance imaging procedures are the best studies for making a definitive diagnosis (2). The CT scan shows subperiosteal hypodensity in the talar neck, with or without a central calcification corresponding to the nidus. It shows an absence of periosteal reaction which is typical in osteoid osteoma of the long bones. The MRI examination demonstrates a decreased intensity on T1, moderately increased signal on the T2-image of the lesion, surrounded by a marginal osteosclerosis with decreased intensity on the different sequences. A central gadolinium hold, represents the osteoid osteoma. It is associated with synovial thickening, intra-articular extrusion, and a marked inflammatory reaction in bone (3,4,5). The scintigraphy tehnique represents an unspecific but sensitive method of diagnosis in the early stages. The osteoid osteoma is visible as a "hot spot" or, in the subperiosteal type, as a diffuse accumulation. Once the diagnosis is confirmed, percutaneous computed tomography-guided thermocoagulation is the most frequently used therapy. En bloc resection and an autogenous bone graft can cure the disorder(5). Localization by computed tomography-guided needle placement or intraoperative radionuclide scanning is recommended to find the lesion for excision (5). The technique of interstitial laser photocoagulation is a safe and cost-effective method of osteoid osteoma treatment (5).
Differential Diagnosis List
Final Diagnosis
Osteoid osteoma in the talar neck.
Liscense
Figures
A conventional X-ray of the left ankle

Ultrasonography, sagittal view of the left ankle

Sagittal MRI slices of the left ankle



A sagittal CT reconstruction
Medical Imaging Analysis Report
I. Radiographic Findings
From the provided ankle X-ray, CT, and MRI images, the following findings are observed:
- A focal lesion in the talar neck region (adjacent to the ankle joint) with localized sclerotic margins.
- On X-ray, a small, well-demarcated lucent focus (possibly with central calcification) is visible within the talar neck, surrounded by sclerotic bone changes. No significant extensive bone destruction or widespread periosteal reaction is observed.
- On MRI, the lesion demonstrates relatively low signal intensity on T1-weighted images and intermediate to high signal intensity on T2-weighted images. Pronounced bone marrow edema and mild inflammatory changes in the joint soft tissues are observed around the lesion.
- CT scan more clearly reveals the low-density lesion (suspected “nidus”) in the talar neck, with a marked sclerotic border.
- There is a small degree of swelling in the local soft tissues, and a small joint effusion may be present, indicating inflammatory irritation.
II. Potential Diagnoses
Considering the patient’s age of 18, marked nighttime pain that is relieved by aspirin, and the above radiographic findings, the following differential diagnoses should be considered:
- Osteoid Osteoma
Typically occurs in adolescents and young adults, characterized by significant nocturnal pain that responds to NSAIDs (e.g., aspirin). Imaging usually shows a small lucent focus (nidus) with a sclerotic border, approximately 1 cm in size. - Osteoblastoma
Similar to osteoid osteoma as both are osteogenic tumors, but osteoblastoma lesions are usually larger (often >2 cm). If imaging demonstrates a substantially larger lesion, this should be considered. - Chronic Osteomyelitis or Subacute Infection
Less common, but should be ruled out in cases of persistent pain or elevated inflammatory markers. CT imaging typically shows bone destruction, sequestra, or sinus tracts. - Stress Fracture
Should be considered in individuals with heavy physical activity or repetitive weight-bearing. However, it typically presents with linear cortical changes or stress reactions, lacking the classic small lucent focus and sclerotic rim.
III. Final Diagnosis
Based on the patient’s nocturnal pain, significant relief with aspirin, and imaging findings showing a “nidus”-like lucent lesion at the talar neck with surrounding sclerosis, the most likely diagnosis is:
Osteoid Osteoma
IV. Treatment and Rehabilitation Plan
- Treatment Strategies
- Conservative Management: Use of NSAIDs (such as aspirin or ibuprofen) to relieve pain and inflammation. This is suitable for patients with small lesions and obvious symptom relief.
- Minimally Invasive Ablation: CT-guided radiofrequency ablation (RFA) or laser photocoagulation, which can be done under local anesthesia or mild sedation, resulting in minimal trauma and quick postoperative recovery.
- Surgical Excision: For significant symptoms or if imaging shows a specific location or larger lesion unsuitable for minimally invasive ablation, consider en bloc surgical resection and bone grafting if necessary.
- Rehabilitation and Exercise Prescription
- Early Stage (1–2 weeks post-treatment or post-surgery): Focus on protecting the affected limb and reducing weight-bearing. Simple passive ankle joint movements or light non-weight-bearing range-of-motion exercises are recommended, avoiding strenuous movements.
- Intermediate Stage (2–6 weeks): Gradually introduce active ankle exercises and mild resistance training, such as using resistance bands for dorsiflexion, plantarflexion, and inversion/eversion exercises. Each session can last 15–20 minutes, 1–2 times per day, with gradual increases in intensity.
- Late Stage (after 6 weeks): Once bone healing is relatively stable and pain is well controlled, progressively resume full weight-bearing functional training. Low-impact aerobic activities such as stationary cycling or swimming can be performed 3–5 times a week, 20–30 minutes each time, with gradual progression to moderate intensity.
- Strength and Stability Training: Incorporate proprioceptive training and ankle stability exercises to further enhance the strength and coordination of the ankle joint and surrounding muscle groups, reducing the risk of recurrence or injury.
Throughout the rehabilitation process, the FITT-VP principle (Frequency, Intensity, Time, Type, Volume/Progression) should be followed, and the regimen should be individualized. If pain intensifies or other discomfort arises, reassessment and adjustment of the training plan are necessary.
V. Disclaimer
This analysis report is for reference purposes only and cannot replace an in-person consultation or professional evaluation by a physician. Patients should combine clinical presentation, laboratory examinations, and professional medical advice to determine the most appropriate treatment plan.
Human Doctor Final Diagnosis
Osteoid osteoma in the talar neck.