Rare case of tibial adamantinoma in 10-year-old immature skeleton



Clinical History
10-year-old male patient presented with an 18 month history of pain and swelling of the left tibia.
Imaging Findings
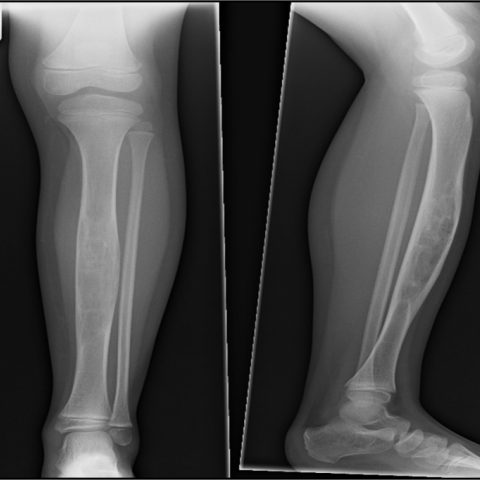
Plain radiograph of the left leg demonstrates grossly expansile lytic lesion involving the tibial diaphysis with invasion of the medullary cavity, ill defined zone of transition. No periosteal reaction, cortical destruction or soft tissue involvement is seen on the plain radiograph.
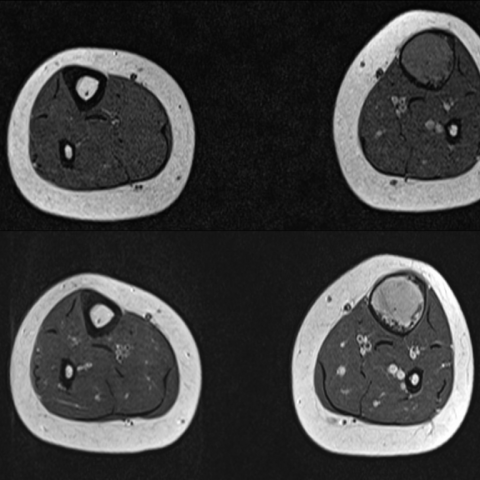
MRI examination confirms a low signal intensity T1 lesion with high signal on FLAIR and a homogeneous enhancement, post gadiolinium. There is complete invasion of the central medullary cavity. No skip lesions were identified.
Bone scintigraphy shows a solitary lesion at this site with increased radiotracer activity. The differential diagnosis at this stage included monostotic fibrous dysplasia, osteofibrous dysplasia and an adamantinoma (rare lesion in immature skeleton). An intralesional resection was performed with samples sent for histopathological analysis.
Histology of the specimen revealed osteo-fibrous matrix with solid nests of cytokeratin positive epithelial cells, findings in keeping with adamantinoma.
Discussion
Adamantinomas are relatively rare tumours accounting for approximately 0.1 to 0.4% of all primary bone tumours. These are considered to represent the aggressive end of the spectrum of fibro-osseous bone tumours, osteo-fibrous dysplasias representing the benign end. Unsurprisingly, given the wide variation in biological activities of these two conditions, the treatment options and overall management vary widely. Whilst adamanatinomas are treated radically with wide local excision, osteofibrous dysplasias can be closely monitored through regular follow up. Despite the cross-over of imaging findings of these related conditions, it is absolutely important that clinicians get the diagnosis right to avoid inappropriate surgical intervention, particularly in young patients.
Adamantinoma is a disease that commonly occurs in the 2nd and 3rd decades of life, although this has been reported in patients as young as 2 years of age. There is a particular prediliction for mid tibial diaphysis. Other long bones such as humerus, radius, ulna and femur can be rarely involved.
Biologically these are aggressive in nature and seen as expansile, lytic lesions on plain radiographs, with ill-defined moth eaten margins. They can be multifocal and can cause surrounding cortical destruction with involvement of the surrounding soft tissue swelling. Metastases to the lung have also been reported.
MRI is regarded as a very useful tool in evaluating the extent of the lesion and in aiding pre-surgical planning for assessment of potential resection margins. Complete invasion of the medullary cavity is the most important differentiating imaging feature of adamantinoma in comparison to osteofibrous dysplasia which commonly tends to confine itself to the cortex of the bone. Age of the patient is also an important differentiating factor, with osteofibrous dysplasias more commonly occurring in immature skeletons, particularly in children less than 10 years of age.
Adamantinomas commonly occur in fused mature skeletons. However, it is important to realise that this is not absolute as shown in the above case study. Besides, there can be considerable cross-over of imaging findings in atypical adamantinomas and osteofibrous dysplasias, for which the treatment and management options can vary widely. Whenever the imaging findings do not tie up with age and clinical presentation, threshold for performing a biopsy of the lesion for histopathological analysis should be low.
Differential Diagnosis List
Final Diagnosis
Adamantinoma
Liscense
Figures
Plain radiographs left leg
MRI

MRI
Nuclear Medicine Bone scan

Medical Imaging Analysis Report
1. Imaging Findings
Based on the provided X-ray and MRI images of the left tibia, there is a notable osteolytic destruction and expansile lesion in the tibial shaft. The lesion boundaries are poorly defined, and “moth-eaten” edges can be observed. In some regions, the cortex appears thinned or even destroyed. On MRI T1-weighted and T2-weighted sequences, the lesion spans a large area, with heterogeneous signal changes within the medullary canal, suggesting it has involved or invaded the bone marrow cavity. Surrounding soft tissues also show a certain degree of involvement and swelling. A bone scan indicates increased radiotracer uptake in the left tibial shaft, suggesting active local bone metabolism.
2. Possible Diagnoses
- Adamantinoma
- Typically arises in the tibial shaft or the metaphyseal-diaphyseal region, commonly in young adults but can also be seen in younger patients.
- Exhibits aggressive growth, can invade the marrow cavity and involve soft tissue. Radiologically, it may present with an expansile osteolytic lesion, often displaying “moth-eaten” bone destruction and soft tissue swelling.
- Osteofibrous Dysplasia
- Commonly seen in children, often confined to the tibial cortex and can present as an expansile cortical change.
- It usually does not extend extensively into the medullary cavity. A lesion that fully involves the marrow cavity is less typical for this entity.
- There is some radiological overlap with Adamantinoma, and differentiation often requires correlation with clinical age and histopathological findings.
- Other Tibial Tumors or Tumor-like Lesions
- Includes entities like Ewing sarcoma or osteosarcoma. However, based on clinical presentation and imaging features, these seem less likely in this case.
3. Final Diagnosis
Considering the patient’s age (10 years), the duration of localized pain and swelling (18 months), and the imaging findings (involvement of the medullary canal with expansile bone destruction), Adamantinoma is a strong possibility despite the pediatric age group. The lesion appears to involve the full thickness of the marrow cavity, which supports this consideration.
However, there is some radiological overlap between Adamantinoma and Osteofibrous Dysplasia, and the patient is relatively young. Therefore, a prompt biopsy and histopathological examination are recommended for definitive diagnosis. If confirmed as Adamantinoma, a more aggressive treatment strategy should be considered.
4. Treatment Plan and Rehabilitation
4.1 Treatment Strategies
- Surgical Treatment: Once histology confirms Adamantinoma, the usual approach involves a wide surgical excision due to its aggressive nature, potentially followed by reconstruction or grafting if needed. For confirmed Osteofibrous Dysplasia, monitoring or limited surgery might be adequate depending on lesion extent and symptoms.
- Preoperative Assessment: Prior to extensive surgical resection, it is crucial to evaluate the patient’s skeletal maturity, fixation strategy, and potential functional deficits.
- Adjuvant Therapy: In cases with soft tissue invasion or specific pathological manifestations, radiotherapy or adjuvant therapy may be considered. However, benefits and risks must be weighed carefully in pediatric skeletal and soft tissues.
- Regular Follow-up: Whether the case is Adamantinoma or Osteofibrous Dysplasia, ongoing monitoring postoperatively or during follow-up is essential to detect local progression, recurrence, or distant metastasis.
4.2 Rehabilitation/Exercise Prescription
Rehabilitation should be carried out under the guidance of orthopedic and rehabilitation specialists, with a gradual, individualized plan. For pediatric patients with such tibial lesions, the following principles (FITT-VP) can be referenced:
- Frequency: Depending on the surgery and lesion extent, start with rehabilitation sessions 2-3 times per week, gradually increasing to 3-5 times per week as recovery progresses.
- Intensity: Focus on low to moderate intensity exercises, avoiding high-impact and excessive weight-bearing activities such as running or jumping. Early stages may include non-weight-bearing or partial weight-bearing exercises, advancing progressively.
- Time: Each session can last 15-30 minutes, adjusted based on tolerance and bone healing. A rehabilitation evaluation should be performed every few weeks to adjust the duration.
- Type: Emphasize range-of-motion exercises and lower-extremity strengthening, gradually incorporating balance and coordination practices. Low-impact activities such as swimming or stationary cycling can be used as supplemental training.
- Progression: Once the lesion shows signs of healing and bone strength is restored, gradually increase weight-bearing and strength training. Any progression should be medically evaluated beforehand.
- Precautions: If the patient experiences increased local pain, redness, or functional difficulties, seek medical attention promptly. High-intensity or high-load exercises should be approached cautiously. Orthoses or supports can be used during rehabilitation to prevent excessive stress on the affected site.
Disclaimer
This report is based on the provided history and imaging findings and serves only as a reference for analysis. It does not replace in-person consultation or professional medical advice. In the event of any doubts, please consult a specialist for personalized diagnosis and treatment planning.
Human Doctor Final Diagnosis
Adamantinoma