Phalangeal microgeodic syndrome in adolescence



Clinical History
A 14-year-old boy with no prior medical history presented with a two-week history of soft tissue swelling on the second phalanx of his left index finger. He reported mild tenderness, minimal redness, and no local warmth. Additionally, he mentioned exposure to cold weather. The consultation took place during wintertime.
Imaging Findings
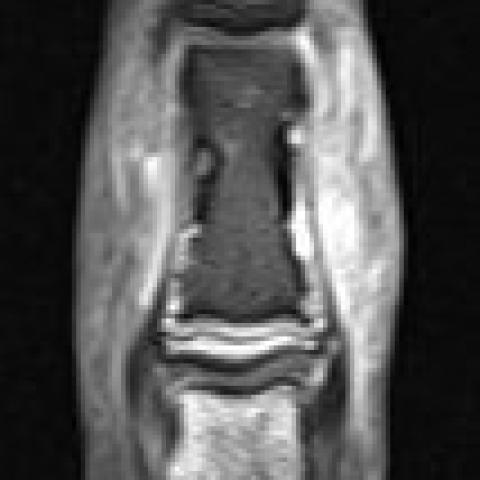
An X-ray revealed small radiolucent areas in the middle phalanx, focal periostitis, and soft tissue swelling. The patient underwent a contrast-enhanced MRI, which demonstrated small lytic cortical bone lesions enhancing with contrast, a diffuse hypovascular appearance of the bone marrow with decreased T1 signal and increased signal on DP fat sat sequences, as well as soft tissue swelling with oedema in the regional area. An ultrasound examination revealed oedema with increased subcutaneous and dermal vascularity and cortical irregularities in correlation with the X-ray findings.
A fluoroscopy-guided biopsy showed bone necrosis without atypia.
A follow-up X-ray showed advanced reparative signs at 7 months from the onset of symptoms.
Discussion
Phalangeal microgeodic syndrome in childhood and adolescence is a rare and benign condition characterized by the formation of small cavities in the phalanges of the fingers [1]. It was first reported in 1970 in a series of 5 cases [2].
Pathophysiology
While not fully understood, it is suggested to involve bone resorption and destruction in response to exaggerated peripheral circulatory impairment following exposure to cold. Cooling is believed to be a significant triggering factor, as the disease tends to manifest during cold months [1]. Persistent swelling of the affected finger with mild pain is a common presenting symptom [3]. This is consistent with the patient's history in our case, as the symptoms occurred during the winter, and upon specific questioning, he reported direct exposure to cold weather on his hands.
Diagnostic Pearls
The key radiographic finding is the observation of multiple small, well-defined, round osteolytic areas that resemble geodes in the medullary and cortical regions of the affected phalanges; these lesions tend to be larger in the proximal metaphysis, as reported. Cortical irregularities and periosteal reaction can also be observed in the affected phalanges, without bone expansion [1,4,5]. Diagnosis can be established based on a compatible clinical history and X-ray, but given the rarity of this condition, additional studies such as MRI, biopsy, or nuclear medicine scans are often requested [6]. The most common MRI findings include low signal intensity in the bone marrow of the affected phalanges on T1-weighted images and high signal intensity on fat-suppressed T2-weighted images. Soft tissue oedema adjacent to the affected bone is also frequently present, suggesting an associated inflammatory response [4].
Prognosis
Regarding treatment, most cases of this syndrome resolve spontaneously within weeks to months, requiring no medical intervention and resulting in no long-term consequences [1,3]. This was also the case with our patient, who only received analgesia for the mild pain he experienced.
Awareness of this condition is crucial to prevent unnecessary diagnostic studies and treatments [6].
All patient data have been completely anonymised throughout the entire manuscript and related files.
Differential Diagnosis List
Final Diagnosis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures


















Imaging Findings
Based on the provided imaging data of the second phalanx (proximal or middle phalanx) of the left index finger, the X-ray shows multiple relatively well-defined roundish radiolucent areas in the mid-shaft and metaphyseal region. Surrounding bone appears slightly sclerotic or irregular, with some irregularity of the cortical bone but no significant bony expansion or marked bone destruction.
MRI sequences (including T1, T2, and fat-suppressed sequences) reveal that the lesion within the involved phalanx appears as low signal on T1 and high signal on fat-suppressed and T2 sequences, indicating bone marrow edema or inflammatory reaction. In addition, there is mild soft tissue edema, but no obvious abscess or other signs of destructive lesions. Overall, the changes are limited to a single phalanx without clear evidence of multifocal involvement or distant spread.
Potential Diagnoses
- Phalangeal Microgeodic Syndrome
Rationale: This condition commonly affects children and adolescents, involving the appearance of multiple small round radiolucent areas in the affected phalanges. It is often triggered by cold exposure or during cold seasons, manifesting primarily as mild swelling, pain, or discomfort in the local area. Imaging typically shows several small cystic radiolucent lesions and mild marrow edema. Generally, the condition is benign with a strong tendency toward spontaneous resolution. - Infectious Lesion (e.g., Chronic Osteomyelitis of the Phalanx)
Rationale: Radiolucent areas in the phalanx could be related to bone destruction caused by infection. In low-grade chronic infections, small areas of bone destruction and surrounding soft tissue edema might be found. However, in this case, there are no clear clinical signs of infection (such as fever or prominent local redness, warmth, and severe pain), nor are there typical radiologic features like sequestrum, involucrum, or a ring of sclerosis. - Benign Bone Tumor or Tumor-Like Lesion (e.g., Bone Cyst, Enchondroma)
Rationale: When multiple cystic lucencies are seen in the phalanges, the possibility of a rare, multiple benign bone lesion should be considered. Nevertheless, these lesions typically appear as solitary lesions or have characteristic morphologic features (such as cartilage calcification). In contrast, the appearance and distribution in this case are more consistent with Phalangeal Microgeodic Syndrome.
Final Diagnosis
Taking into account the patient’s age (adolescent), clinical presentation (mild local swelling and pain without significant inflammatory signs), imaging findings (multiple small cystic radiolucent foci confined to the phalanx, mild bone marrow edema, minimal soft tissue swelling), and the tendency to appear after cold exposure or worsen in winter, the most likely diagnosis is Phalangeal Microgeodic Syndrome. This condition is a benign and self-limiting disease that typically resolves progressively over several weeks to months with a generally favorable prognosis.
Treatment Plan and Rehabilitation
1. Treatment Strategies
- General Management: Most cases do not require specialized treatment. For mild symptoms, supportive care is sufficient, including keeping the affected area warm and avoiding further cold exposure.
- Pain Control: For mild pain, oral or topical analgesics such as acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs) may be used to relieve discomfort.
- Observation and Follow-Up: Regular imaging follow-up is recommended to monitor whether the lesions gradually resolve or improve, which typically occurs within a few weeks to several months. If symptoms significantly worsen or new symptoms appear, other malignant or infectious causes should be ruled out.
2. Rehabilitation Exercises and Exercise Prescription
- Rehabilitation Principles: Once the acute symptoms subside, gradual hand function exercises can be performed to maintain and improve joint flexibility of the fingers, preventing stiffness or muscle atrophy from prolonged immobilization.
- FITT-VP Principle:
- Frequency: Begin with 3–4 sessions per week, increasing to 5–6 sessions as symptoms improve.
- Intensity: Exercise should not cause significant pain and should only result in mild discomfort at most. Avoid high-intensity activities.
- Time: Start with 10–15 minutes of exercise per session, gradually increasing to 20–30 minutes.
- Type: Possible activities include using a grip ball, active and passive flexion-extension of the finger joints, and fine motor tasks (e.g., picking up small beans or marbles).
- Volume: As symptoms improve, total weekly training time can be increased by 10–20% incrementally.
- Progression: Once local pain and swelling have significantly improved, the difficulty of hand function training can be slightly increased, such as longer grip exercises or more challenging dexterity training.
Disclaimer
The above analysis report is based on the available clinical and imaging data and is intended for reference only. It does not replace in-person consultation or professional medical advice. If you have any concerns or if your condition changes, please seek further medical evaluation and treatment promptly.
Human Doctor Final Diagnosis