Kiloh-Nevin syndrome



Clinical History
A 48-year-old woman with no history of a single trauma presented with pain in the right forearm and loss of flexion at the distal interphalangeal joint of the index finger and interphalangeal joint of the thumb. Magnetic Resonance Imaging (MRI) of the elbow and wrist was requested (Fig. 1-4).
Imaging Findings
Increased signal intensity is depicted on fat-suppressed T2-weighted images (WI) in keeping with muscle oedema in the radial half of the flexor digitorum profundus, the flexor pollicis longus and the pronator quadratus muscles (Fig. 1-3). Furthermore, fatty infiltration and atrophy is seen on the T1-WI (Fig. 4). These imaging findings are consistent with subacute to chronic denervation of the anterior interosseous nerve (AIN). No compression or entrapment of the nerve could be demonstrated. Diagnosis of a complete interosseous syndrome was made.
Discussion
The AIN syndrome or Kiloh-Nevin syndrome arises when the AIN is entrapped or compressed in the proximal part of the forearm.
The AIN is a motor branch to the deep ventral muscles of the forearm originating from the median nerve approximately 8 cm distal to the lateral epicondyle. This branch innervates the flexor pollicis longus, the radial half of the flexor digitorum profundus and the pronator quadratus muscles. An incomplete AIN syndrome arises when there is selective involvement of nerve bundles that innervate the flexor pollicis longus or the flexor digitorum profundus muscles with or without involvement of the pronator quadratus muscle [1].
The most frequent causes are direct traumatic damage and external compression. Traumatic causes are often the result of iatrogenic actions such as venous injection, puncture, surgery and cast pressure. A soft tissue tumour, congenital anomalies and vascular abnormalities are the most frequent causes of external compression [1, 2].
Typical clinical features are a dull pain in the volar region of the forearm and an acute onset of muscle weakness which affects the thumb, index finger and occasionally the middle finger. The ‘circle sign’, ‘O-sign’ or ‘Spinner sign’ is pathognomonic [3]. Patients cannot form the letter “O” with their index finger and thumb. Flexion at the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger is not possible due to lack of innervation of the flexor pollicis longus or flexor digitorum profundus muscles. Since the AIN is purely a motor branch, numbness of the skin is not an accompanying symptom.
MRI is the imaging modality of choice. In the (sub)acute stage an increased signal intensity is seen in the flexor digitorum profundus, flexor pollicis longus and pronator quadratus muscles on fatsuppressed T2-WI or STIR images. In a more chronic stage, T1-WI show fatty infiltration and atrophy of the corresponding muscles. Isolated signal changes of the pronator quadratus muscle need to be interpreted with caution. Slight hyperintensity on T2-WI or STIR-images is often seen in asymptomatic individuals. Therefore, the combination of signal intensity changes in different muscles innervated by the AIN is required for the diagnosis.
Surgical intervention should be considered in patients where the clinical data suggest a compression neuropathy or a transection of the nerve. Otherwise, conservative measures (physical therapy and non-steroidal anti-inflammatory drugs) are recommended for a minimum of 12 weeks. Spontaneous recovery one year after the onset has been reported [1, 2].
Differential Diagnosis List
Final Diagnosis
Anterior interosseous syndrome (Kiloh-Nevin syndrome)
Liscense
Figures
Axial fat-suppressed T2-WI

Axial fat-suppressed T2-WI
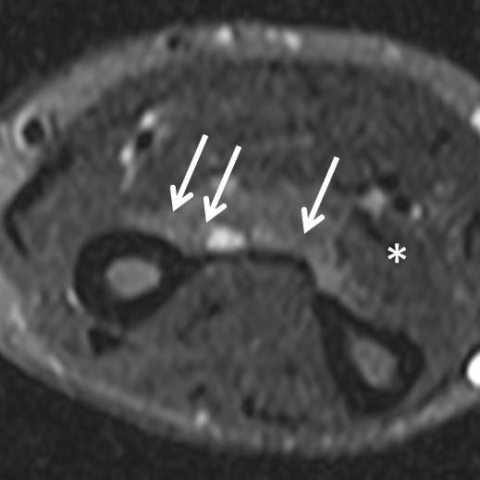
Axial fat-suppressed T2-WI

Axial T1-WI

Medical Imaging Analysis Report
I. Radiological Findings
Based on the provided forearm MRI images (T2WI/STIR and T1WI), the following findings can be observed:
- In the proximal to mid forearm, within the radial-side deep flexor muscle group (mainly including the flexor pollicis longus muscle group and the radial part of the flexor digitorum profundus), T2WI/STIR shows focal or cord-like hyperintense signal changes.
- In some images, the muscle bellies of the flexor pollicis longus and the radial portion of the flexor digitorum profundus may demonstrate localized increased signal; mild muscle atrophy or fatty infiltration can be observed locally (more prominent on T1WI).
- No significant bony abnormalities or obvious structural destruction of the elbow joint; the joint capsule and articular surfaces appear essentially normal.
- No obvious soft tissue tumor or space-occupying lesion is identified; only a slightly narrowed fat space around the nerve area is noted locally.
II. Potential Diagnoses
Considering a 48-year-old female with forearm pain and flexion dysfunction in the distal interphalangeal (DIP) joint of the index finger and the interphalangeal joint of the thumb, the following differential diagnoses are to be considered:
-
Anterior Interosseous Nerve Syndrome (AIN Syndrome):
Caused by compression or injury of the anterior interosseous branch of the median nerve, affecting only motor fibers. This can present with weakness in flexing the distal interphalangeal joints of the thumb and index finger, typically manifested by an inability to form the “OK sign.” On imaging, the involved muscles (flexor pollicis longus, radial part of the flexor digitorum profundus, and pronator quadratus) may show hyperintense signals on T2WI. This is the most common potential diagnosis. -
Tendon structural injury (e.g., partial tear of the flexor pollicis longus or the flexor digitorum profundus tendon of the index finger):
Partial tendon injuries can lead to similar functional impairments in flexion of the fingers or thumb. However, tendon ruptures typically involve a clear history of trauma or severe pain, and MRI would demonstrate interruption of tendon fiber continuity, which is not fully consistent with this case. -
More proximal lesion of the median nerve:
If the median nerve is compressed at a more proximal site, such as at the elbow or a widespread lesion in the proximal forearm, similar finger and thumb dysfunction may occur. However, this is often combined with sensory involvement (which is not clearly present in this case). -
Other compressive lesions:
Rare soft tissue tumors or vascular anomalies could cause localized nerve compression, but no obvious space-occupying lesion was found on this MRI.
III. Final Diagnosis
Taking into account the patient’s age, the symptoms (weakness in extending or flexing the distal joints of the thumb and index finger, inability to form the “OK sign”), the MRI findings (localized hyperintense signals on T2WI with partial muscle atrophy), and the absence of notable sensory disturbance, the most likely diagnosis is:
Anterior Interosseous Nerve Syndrome (Kiloh-Nevin Syndrome).
If further confirmation is needed, combining electromyography (EMG) to assess nerve innervation of the affected muscles and ruling out rare tumors or vascular malformations is advised.
IV. Treatment Plan and Rehabilitation
Most AIN syndromes are related to nerve compression or localized inflammation, and often exhibit a degree of spontaneous recovery. Therefore, the treatment strategy generally includes:
-
Conservative treatment:
It is recommended to implement conservative management for at least 8–12 weeks, including physical therapy (such as physiotherapy, ultrasound, or soft tissue mobilization), administration of non-steroidal anti-inflammatory drugs (NSAIDs) to alleviate local inflammation and pain, and reducing external compression or repetitive activities. -
Surgical treatment:
If there is clear evidence of compression, a local tumor, or another identifiable compressive lesion, or if no significant improvement is noted after 3–6 months of conservative treatment, surgical decompression or exploration can be considered. -
Rehabilitation and exercise prescription:
For forearm and hand dysfunction, it is recommended to adopt a phased approach to training in order to improve or maintain function of the affected muscle groups:-
Initial Phase (Weeks 1–4):
- Perform light grip training with a soft grip ball: gently squeeze using fingers and thumb, 10–15 repetitions each time, 2–3 sets a day.
- Practice active forearm pronation and supination exercises, starting with small ranges of motion, 2–3 times per day, 10–15 repetitions each time.
- Avoid excessive force or prolonged repetitive movements.
-
Intermediate Phase (Weeks 4–8):
- Gradually increase resistance training, such as using a grip ball or resistance bands, progressively intensifying the load for the forearm muscles.
- Focus on precise flexion exercises targeting the flexor pollicis longus and flexor digitorum profundus (e.g., assisted pinch training between thumb and index finger under the guidance of a therapist).
- Perform these exercises 3–4 times a week for 15–20 minutes each session, progressively increasing intensity.
-
Late Phase (Weeks 8–12 and beyond):
- Once symptoms permit or partial function returns, include refined hand coordination and endurance training (e.g., using putty or finger coordination tools).
- Gradually reintroduce functional exercises based on daily activities, such as various pinch grips between thumb and index finger, in a safe environment.
-
Initial Phase (Weeks 1–4):
The FITT-VP principle (Frequency, Intensity, Time, Type, Volume, Progression) should be adjusted in response to the patient’s rehabilitation progress, under the guidance of a professional therapist or physician.
Disclaimer: The content of this report is solely a reference analysis based on the information provided and cannot replace an in-person consultation or professional medical advice. Patients should consider their actual clinical conditions and proceed with further examinations and treatment under specialist guidance.
Human Doctor Final Diagnosis
Anterior interosseous syndrome (Kiloh-Nevin syndrome)