Subungual epidermoid cyst



Clinical History
A 30-year-old, left-handed male patient, presented with a subungual mass of the third finger of the left hand with secondary nail dystrophy (Fig. 1). The patient did not recall any injury to that finger.
Imaging Findings
Conventional radiography revealed soft tissue swelling with cortical scalloping of the dorsal and ulnar part of the distal phalanx of the third finger (Fig. 2).
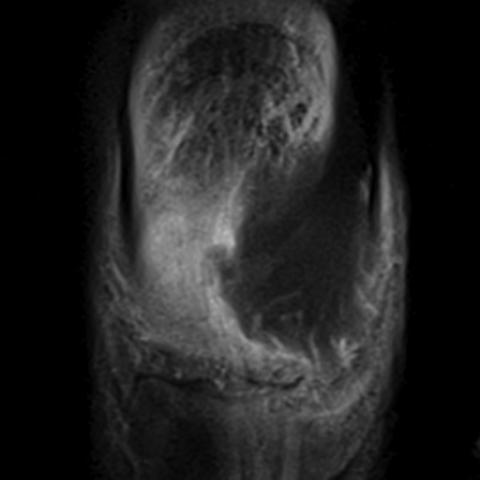
The patient underwent a high resolution 3T MRI of the nail apparatus with coronal and axial SE (spin echo) T1-w (Fig. 3-4), sagittal and axial proton density with fat saturation (Fig. 5-6), axial post gadolinium i.v injection SET1-w (Fig. 7), coronal post gadolinium i.v injection SET1-w with fat saturation (Fig. 8) and 3D VIBE post gadolinium i.v injection with multiplanar reconstructions (Fig. 9).
On MRI, the soft tissue mass corresponds to a medial subungual process within the dermis of the nail bed, iso- or low-intensity on all sequences without enhancement post gadolinium injection compatible with keratinised or fibrous tissue.
The surgical biopsy showed a keratinising cystic lesion with no atypical cells.
Discussion
The epidermoid cyst is a benign cystic lesion related to the proliferation of epidermal cells whose aetiology remains controversial. The two main hypotheses are that of post-traumatic cell implant and that of embryonic cell rest [1].
The locations of intraosseous epidermoid cysts are preferentially described in the skull and distal phalanges of the fingers, especially the distal phalanx of the third finger of the left hand in men as in our case [2].
Clinically, these lesions manifest as a soft tissue swelling that is sometimes warm, tender and red. Deformation of the overlying nail has also been described in subungual locations [2].
In this clinical context, an assessment by conventional radiography is generally prescribed and shows soft tissue swelling, cortical scalloping and possibly well-defined lytic bone lesion with a sclerotic rim. In our institution, we generally complete this assessment by 3T HR MRI which allows us to specify the exact location and signal characteristics of the lesion. The epidermoid cyst typically has an intermediate signal or low signal on all sequences [3].
The differential diagnosis includes kerathoacanthoma, skin carcinomas and fibromas [2, 3]. The keratoacanthoma is a benign tumour characterized by a rapid endoexophytic growth of squamous epithelium with a central keratin-filled crater of low signal intensity on all sequences; because of their similarities keratoakanthoma and squamous cell carcinoma cannot be differentiated at MRI [3]. Fibromas are slow growing lesions composed of thick hypocellular collagen bundles with low signal on all MRI sequences and no contrast enhancement [4].
The diagnosis is confirmed on histology by the presence of a stratified squamous epithelium encapsulated lesion that contains keratinised debris [2].
Surgical resection with curettage of the lesion and its wall reduces the risk of recurrence and is the treatment of choice [5].
In conclusion, the epidermoid cyst is a benign but symptomatic lesion relatively easy to treat and it should be mentioned in the differential diagnosis of lesions in the distal end of the finger, especially in the post-traumatic context.
Differential Diagnosis List
Final Diagnosis
Subungual epidermoid cyst
Liscense
Figures
Photography of the lesion

Conventional radiography

Nail MRI, coronal SET1-w



Nail MRI, axial SET1-w


Nail MRI, sagittal proton density with fat saturation

Nail MRI, axial proton density with fat saturation


Nail MRI, axial post gadolinium i.v injection SET1-w


Nail MRI, coronal post gadolinium i.v injection SET1-w


Nail MRI, 3D VIBE post gadolinium i.v injection

Medical Imaging Analysis Report
1. Imaging Findings
Based on the provided X-ray and MRI images of the third finger on the left hand, the following characteristics can be observed:
- A soft tissue mass under the nail (nail bed area), causing local nail deformity or elevation.
- On the plain X-ray, soft tissue swelling is visible, and there are “shell-like” changes on the distal phalanx, suggesting possible chronic changes causing cortical erosion or compression.
- MRI shows a lesion appearing as a cystic structure with a well-defined margin. On T1- and T2-weighted sequences, it generally demonstrates low or intermediate signal, relatively homogeneous, with localized keratin-like low signal.
- The surrounding soft tissue signal is relatively normal or shows only mild inflammatory changes.
- No obvious fracture lines or severe destruction of the phalanx are observed, primarily indicating slight bony compression of the distal phalanx.
2. Potential Diagnoses
Combining the patient’s history (30-year-old male, no clear history of trauma, local nail deformity and pain) and the imaging findings, possible diagnoses or differential diagnoses include:
- Epidermoid Cyst
- Keratoacanthoma or Squamous Cell Carcinoma
- Fibroma
Often found under the nail, it can appear as a cystic or solid-cystic lesion. On imaging, it commonly displays low or intermediate signal. Due to the presence of keratin, it may show areas of low or heterogeneous signal within the cyst, and can lead to nail deformity or damage.
These two conditions can be difficult to differentiate on MRI, both presenting as localized soft tissue masses. Nail plate destruction or a “crater-like” structure may be visible. Differences in growth rate and local aggressiveness are key points of clinical concern.
Often a slow-growing solid lesion. On MRI, it typically appears as low signal, with minimal or no enhancement, and tends to be relatively firm in texture.
3. Final Diagnosis
Considering the patient’s age, the benign growth pattern affecting the nail, the cystic lesion on MRI, and its typical location at the fingertip, the most likely diagnosis is: Epidermoid cyst. A definitive diagnosis can usually be confirmed during surgery and through pathological examination.
4. Treatment Plan and Rehabilitation
4.1 Treatment Plan
- Surgical Treatment: For patients with significant symptoms or severe nail deformity, complete surgical excision of the cyst along with thorough curettage of the cyst wall is the primary approach. Bone remodeling may also be performed to reduce recurrence risk.
- Conservative Treatment: If the lesion is small and symptoms are mild, observation is an option. Regular follow-up is necessary, and surgery may be considered if pain worsens or further nail deformity develops.
- Postoperative Management: Depending on the size of the surgical wound, free flap coverage or nail bed reconstruction may be needed. Careful infection prevention is crucial.
4.2 Rehabilitation and Exercise Prescription
Postoperative rehabilitation exercises are necessary to restore local function and prevent scar formation or joint stiffness. Following the FITT-VP principle, the rehabilitation can be divided into stages:
- Early Postoperative Phase (approximately 1–2 weeks)
- Focus on wound healing; keep the affected finger elevated and reduce water exposure to prevent infection.
- After dressing removal, begin gentle finger movements progressively, avoiding excessive traction on the wound.
- Intermediate Rehabilitation Phase (approximately 2–4 weeks)
- Increase daily finger activities, practicing simple fist clenching and finger extension exercises. The range should not cause significant pain, and intensity can be gradually increased.
- Each session lasts around 10–15 minutes, conducted 2–3 times a day.
- Later Strengthening Phase (approximately 4–6 weeks and beyond)
- If the wound has healed well, larger movements of the finger can be practiced, such as squeezing a rubber ball or pinch strength exercises.
- Include finger flexibility exercises and flexion-extension resistance training to avoid adhesions and stiffness.
- The frequency can gradually increase to 3–4 times per day, about 15 minutes per session, adjusting as tolerated.
If the patient has other special conditions (such as osteoporosis or compromised hand blood supply), exercise intensity should be appropriately reduced, and monitoring should be increased to ensure safety.
Disclaimer: This report is a reference analysis based on the available imaging and patient history. It cannot replace a face-to-face diagnosis or the opinion of a professional physician. Any treatment or rehabilitation decision should be made in conjunction with clinical examination and specialized medical evaluation.
Human Doctor Final Diagnosis
Subungual epidermoid cyst