Chondroid syringoma of the foot



Clinical History
A 59-year-old woman presented with a plantar foot mass that is present for 15 years. She has a history of a tumour debulking surgery 12 years ago. The mass is painful when standing or walking.
Imaging Findings
Radiographs demonstrate well-defined erosions of the cuboid, navicular, anterior calcaneus, and intermediate and lateral cuneiforms.
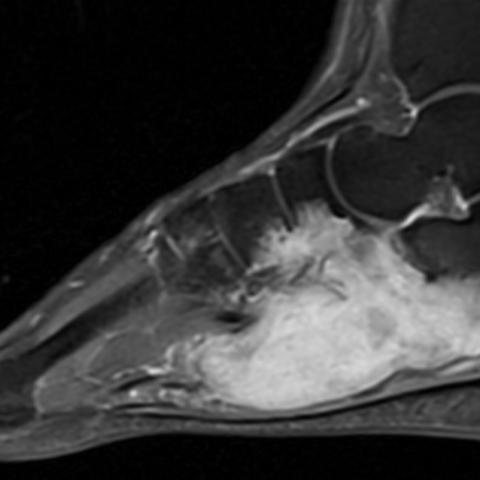
Axial PD FS and sagittal T2 FS MR images demonstrate a lobulated, mildly heterogeneous, hyperintense lesion in the deep plantar soft tissue of the foot, with erosion into the surrounding bones. The mass has heterogeneous, primarily low T1 signal intensity. The mass partially encases the flexor hallucis longus and flexor digitorum longus tendons. Contrast-enhanced T1 images show diffuse enhancement of the mass.
Histopathology images at low and high magnification show nests of epithelioid cells on a background of myxoid and chondroid stroma.
Discussion
Chondroid syringoma (CS), also known as cutaneous mixed tumour, is a skin appendageal tumour of sweat gland origin, usually found in the head and neck region and much less commonly found in the extremities [1]. CS has an incidence of <0.098% and most commonly affects middle-aged or older males [2]. CS is morphologically identical to pleomorphic adenoma of the salivary glands.
The typical presentation is a slow-growing, firm nodule in the dermis or subcutaneous fat. Prior case reports have shown a heterogeneous T2 hyperintense and T1 hypointense mass on MRI, with enhancement following contrast administration [1,2]. While it is most commonly benign, rare cases have been shown to be malignant [3]. Since malignant CS is uncommon, there are currently no concrete criteria to determine benign versus malignant CS when analyzing histopathology [4].
At pathology, there is extensive chondroid and/or myxoid stroma, with nests of epithelioid cells that have abundant eosinophilic cytoplasm and vesicular nuclei [5].
Whether benign or malignant, it has been found that surgical excision with wide margins is often curative [5], with no requirement for radiation or systemic therapy for benign disease. Once excised, the sample can be analyzed for evidence of malignancy. Although there are no well-defined criteria for malignant CS, findings such as pleomorphism, mitoses, and cytoplasmic atypia may indicate malignancy [3]. Adjuvant radiation therapy has been utilized in the treatment of rare malignant tumours [3]. In this case, there were no features of malignancy, and the patient had no evidence of tumour recurrence on one-year follow-up MRI.
As a skin appendageal tumour, chondroid syringoma is uncommonly a radiologic diagnosis. However, due to the potential for deep growth, CS can be included in the differential diagnosis for an infiltrative mass in the extremities.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Benign chondroid syringoma
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Lateral radiograph

PA and oblique radiographs

Sagittal T2 fat sat

Axial PD fat sat

Coronal T1 without and with contrast

Sagittal T1 fat sat with contrast
H&E stain at 40x

H&E stain at 200x

Medical Analysis Report
1. Imaging Findings
A soft tissue mass shadow is visible in the patient’s right plantar region, with relatively clear boundaries. There is local soft tissue proliferation accompanied by varying degrees of swelling. X-ray imaging shows that the continuity of the metatarsal and tarsal bones is intact, without obvious signs of bone destruction or fracture, and a dense shadow can be seen in the adjacent soft tissue. MRI indicates the lesion is located within the plantar soft tissue layer, presenting low or iso-intensity on T1-weighted sequences and high signal intensity on T2-weighted sequences. Contrast-enhanced scans show marked enhancement, suggesting certain soft tissue tumor characteristics.
2. Possible Diagnosis
- Chondroid Syringoma (Mixed Tumor of Soft Tissue): Based on the long-term presence of the lesion, slow growth, postoperative recurrence, and the cartilaginous or mixed high signal on MRI, combined with pathological findings indicating skin appendage origin (including cartilaginous and epithelial components), these features are consistent with chondroid syringoma.
- Other Skin Appendage Tumors: Such as eccrine sweat gland adenoma or sebaceous adenoma, which are rare but can also present as a slowly growing superficial soft tissue mass.
- Neurogenic Tumors: Such as schwannomas, which can also appear as slowly enlarging, well-defined soft tissue masses. However, in this case, the imaging and postoperative pathology are not entirely consistent with a typical neurogenic tumor.
- Synovial-Origin Soft Tissue Lesions: These may occur in the foot or around other joints, but histologically they usually show synovial or myxoid components, which differs from the evident cartilaginous and epithelial components seen in this case.
3. Final Diagnosis
Considering the patient’s age, clinical presentation (chronic plantar foot pain, pain while standing and weight-bearing), surgical history, imaging findings (high T2 signal and significant contrast enhancement), and pathological results (presence of cartilaginous matrix and skin appendage epithelial components), the most likely diagnosis is Chondroid Syringoma (Mixed Tumor of Soft Tissue). Currently, the lesion shows benign characteristics with no clear signs of malignancy.
If the lesion enlarges again, pathology indicates malignancy, or recurrence is observed, further evaluation or a more extensive resection, possibly combined with radiation therapy, may be considered.
4. Treatment Plan and Rehabilitation
Treatment Strategy:
- Surgical Treatment: For confirmed or highly suspected benign mixed tumors, complete surgical excision with adequate margins is the principal treatment to reduce the risk of recurrence.
- Postoperative Follow-Up: It is recommended to follow up regularly, especially within the first year, including reviewing clinical symptoms and imaging (e.g., MRI) to detect any potential recurrence as early as possible.
- Malignant Potential: If intraoperative or postoperative pathology suggests malignant features (significant cell atypia, disorganized tissue structure, active proliferation), radiation therapy or additional adjuvant treatments may be required.
Rehabilitation and Exercise Prescription (FITT-VP Principle):
-
Early Postoperative Phase (Tissue Healing):
- Frequency: 1–2 sessions per day of light functional activity training, focusing on plantar flexibility and gentle joint mobility exercises.
- Intensity: Low intensity, avoiding significant pain. Emphasize simple exercises such as ankle plantarflexion/dorsiflexion and toe gripping.
- Time: 5–10 minutes per session, adjusted according to patient tolerance.
- Type: Conduct gentle ankle and toe activities while seated or lying down, avoiding excessive tension on the surgical site.
- Volume/Progression: Once the wound is well-healed and pain is controlled, gradually increase the frequency or length of the activity sessions.
-
Intermediate Rehabilitation Phase (Muscle Strength & Stability):
- Frequency: 3–4 times per week.
- Intensity: Gradually increase to moderate intensity; commence lower limb weight-bearing activities such as supported standing balance exercises (using a wall or crutches for assistance).
- Time: 15–20 minutes per session, with rest periods between sets.
- Type: Focus on ankle strength and stability exercises (e.g., elastic band resistance exercises), short-distance walking practice, gradually increasing plantar weight-bearing duration.
- Volume/Progression: Advance to heel raises, toe stands, and gentle squats based on individual recovery.
-
Late Rehabilitation Phase (Functional Return to Activity):
- Frequency: 3–5 times per week.
- Intensity: Primarily moderate intensity, transitioning to a slightly higher intensity level under professional guidance.
- Time: 30–45 minutes each session, gradually restoring daily activities (such as walking on flat surfaces, climbing stairs).
- Type: Incorporate core and lower-extremity strengthening exercises to improve balance and coordination, such as balance board training, light jogging, or stationary cycling (if foot pain is well controlled).
- Volume/Progression: Depending on pain levels and functional recovery, gradually resume normal daily activities and light physical exercise. If there are no significant structural issues with the lower leg or foot, light jogging or aerobic exercise may be attempted under professional guidance.
Important Precautions:
- If you develop local redness, swelling, increased pain, or other symptoms, seek medical attention to rule out wound infection or lesion recurrence.
- If you have osteoporosis or other chronic medical conditions, exercise intensity and weight-bearing should be closely monitored and guided by a healthcare professional.
- Wear appropriate footwear and socks during rehabilitation to prevent excessive irritation or pressure on the surgical site.
Disclaimer: This report is provided for informational purposes only and is not a substitute for in-person medical consultation or professional diagnosis and treatment. If you have any questions or changes in your condition, please seek medical advice promptly.
Human Doctor Final Diagnosis
Benign chondroid syringoma