Myositis ossificans of the anterior chest wall



Clinical History
A 36-year-old active man presents with a tender lump in the left anterior chest wall. There was no history of trauma. Initial MRI of the anterior chest wall was ordered.
Imaging Findings
MRI of the chest wall was performed to investigate the mass (Fig. 1). The lesion showed heterogeneously increased T2 signal with a hypointense rim (Fig. 1a). The mass was slightly hyperintense to muscle on T1 sequences (Fig. 1b). The mass measured 3.2 (AP) x 1.9 (craniocaudal) x 3.7 cm (transverse). Surrounding muscle was oedematous, but there was no evidence of invasion into subcutaneous soft tissues or underlying costal cartilage (Fig. 1). Given the nonspecific MRI features, biopsy was ordered to rule out a primary soft tissue tumour.
Ultrasound-guided biopsy was conducted and pathology reported the pathological and radiologic findings were in keeping with myositis ossificans. Follow-up CT imaging was recommended.
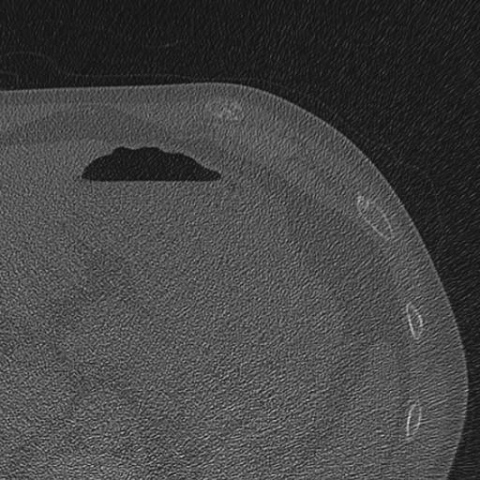
Follow-up CT imaging demonstrated the lesion within the musculature anterior to the costal cartilage (Fig. 2). The lesion was calcified, smaller than previously measured on MRI, and skin tenting was reduced. These findings were consistent with a diagnosis of myositis ossificans.
Discussion
Posttraumatic myositis ossificans (PTMO) is a benign cause of a soft tissue mass which may spontaneously resolve over time. PTMO is the most common subtype of myositis ossificans (MO) and comprises up to 75% of cases [1]. It often occurs in the 2nd or 3rd decade of life with a slight predilection for males [1]. Vastus lateralis and brachialis are the most commonly affected muscles, however, other sites such as pectoralis, gluteal, and intercostal muscles can be affected [2]. Despite its nomenclature, a history of trauma is absent in up to 40% of cases [3].
PTMO often presents as a tender swelling with or without cutaneous erythema, but it can also be clinically asymptomatic. Given the nonspecific clinical picture, physicians rely on diagnostic imaging to delineate MO from infection or malignancy. In our case, MRI of the anterior chest wall was initially ordered to investigate this soft tissue mass.
MRI allows for visualisation of acute lesions prior to calcification. Lesions often appear T1-isointense with or without peripheral enhancement [4]. T2 scanning shows intermediate to high signal and may have a hypointense rim [5]. MRI findings can often be nonspecific, particularly in the early stages when traumatic oedema is present. This was the case with our patient, and the lesion was therefore biopsied. Pathology reports definitively ruled out a malignant lesion and suggested the possibility of MO. CT imaging was recommended for definitive diagnosis.
CT provides valuable additional information in these cases due to its sensitive and accurate depiction of calcium deposition. CT findings vary depending on the maturity of the MO lesion. In early weeks there is soft tissue swelling, but no calcification or ossification. After several weeks, a centrifugal zonal maturing pattern develops and the periphery calcifies. Although uncommon, it is possible for homogenous calcification to occur. This is the most frequent reason for decreased diagnostic confidence [6]. CT imaging will also show local tissue compression without invasion of nearby structures [4]. Finally, CT is able to evaluate periosteal reactions, monitor skin tenting, and track lesion maturation [6]. These factors help to exclude a malignant process and confirm the diagnosis.
Management of MO is usually conservative given that lesions often regress spontaneously. Therefore, recognition of characteristic imaging features is important to avoid unnecessary surgical intervention. This case demonstrates a less commonly encountered site for MO and outlines imaging characteristics to guide definitive diagnosis.
Differential Diagnosis List
Final Diagnosis
Myositis ossificans of the anterior chest wall
Liscense
Figures
MRI imaging of the anterior chest wall


Follow-up CT imaging of the chest wall

Medical Imaging Analysis Report
1. Imaging Findings
This patient is a 36-year-old male who presented with a palpable, tender mass in the left anterior chest wall, with no clear history of trauma. Based on the uploaded MRI images, the following can be observed:
- A soft tissue density/signal abnormality in the soft tissue of the left anterior chest wall, with a relatively regular shape.
- On MRI T1-weighted images, the lesion predominantly appears as an isointense signal, with partial peripheral enhancement. On T2-weighted images, a moderate to high signal can be seen, possibly surrounded by a thin low-signal rim.
- Overall, there is no obvious involvement of adjacent ribs or sternal bone destruction, and no clear evidence of pleural involvement.
Subsequent CT scan results show:
- Calcification or ossification within the lesion, displaying a centripetal or peripheral ring-like pattern of calcification.
- No obvious signs of invasion into adjacent structures. No bone destruction or significant soft tissue mass invasion was observed.
Combined with the pathology report, it was determined to be a benign lesion, ruling out signs of malignancy.
2. Differential Diagnosis
Based on the patient’s clinical presentation (local mass with tenderness) and the imaging features (an early suspicious soft tissue mass on MRI, calcifications in peripheral or irregular patterns on CT), the following differential diagnoses can be considered:
- Myositis Ossificans (including trauma-induced type)
Even in the absence of a clear trauma history, myositis ossificans can occur (statistically, about 40% of patients do not have a definite history of trauma). Typical imaging findings demonstrate soft tissue calcifications, with a characteristic centripetal maturation pattern. - Soft Tissue Sarcoma or Malignant Tumor
Malignant tumors can also present as a soft tissue mass with calcifications; however, calcifications are often irregular, and there may be associated bone destruction or invasion of nearby structures. In this case, based on pathology and further CT assessment, malignancy was ruled out. - Infection/Abscess
Infectious lesions may appear as soft tissue swelling with variable enhancement, and early lesions can be difficult to differentiate from other conditions. However, they can usually be differentiated through clinical inflammatory markers (e.g., WBC count, CRP) and imaging follow-up. This patient had no evident signs of infection or laboratory abnormalities.
3. Final Diagnosis
Taking into account the patient’s age, symptoms, the absence of a significant trauma history yet the presence of a painful mass, in conjunction with the MRI and CT imaging features, and confirmation by pathology that ruled out malignancy, the definitive diagnosis is:
Myositis Ossificans (suspected post-traumatic type despite no clear history of trauma).
4. Treatment Plan and Rehabilitation
Given that myositis ossificans is often self-limiting, most cases may spontaneously resolve or stabilize within several months to 1–2 years. Usually, conservative management is adopted. Specific recommendations are as follows:
- Conservative Treatment:
- In the early stage, non-steroidal anti-inflammatory drugs (NSAIDs) can be used to alleviate pain and inflammation.
- Avoid repeated trauma or excessive pressure on the local soft tissue.
- Regular follow-up imaging to monitor the lesion’s maturation and changes in size.
- Possible Surgical Intervention:
- If the lesion continues to grow or causes functional impairment and significant pain, and conservative treatment is ineffective, surgical excision can be considered.
- Surgical indications require careful evaluation, including lesion maturity and its relationship with surrounding tissues.
- Rehabilitation and Exercise Prescription:
- During the acute phase, avoid strenuous exercise. Opt for low-impact activities, taking care not to aggravate local pain or irritation.
- Once symptoms improve, exercise intensity can be gradually increased following the FITT-VP principle:
- Frequency: 3–4 times per week.
- Intensity: Start with low-resistance training or low-intensity cardio, ensuring it does not exacerbate pain.
- Time: 15–20 minutes per session initially, gradually extending to around 30 minutes.
- Type: Activities such as swimming, resistance band stretching, and core stability exercises can be used to reduce direct impact on the affected area.
- Progression: As pain subsides and function improves, gradually increase resistance or load. Closely monitor local reaction.
- Continue to observe the local soft tissue response. If significant swelling or pain increases, reduce or temporarily stop exercise and consult with a medical professional.
5. Disclaimer
This report is based on the clinical and imaging data provided and is for medical reference only. It does not replace an in-person consultation or the clinical judgment of a professional physician. If you experience any changes in your condition or have concerns, please seek medical attention promptly.
Human Doctor Final Diagnosis
Myositis ossificans of the anterior chest wall