Tensor fascia latae pseudotumour in a setting of abductor tendinopathy



Clinical History
A 68-year-old woman presents to the radiology department with pain in her right hip and knee. She reports that the pain began approximately 12 months ago, with a marked worsening over the past six months. She now presents with a palpable mass on the lateral aspect of her right thigh. There is no evident history of trauma.
Imaging Findings
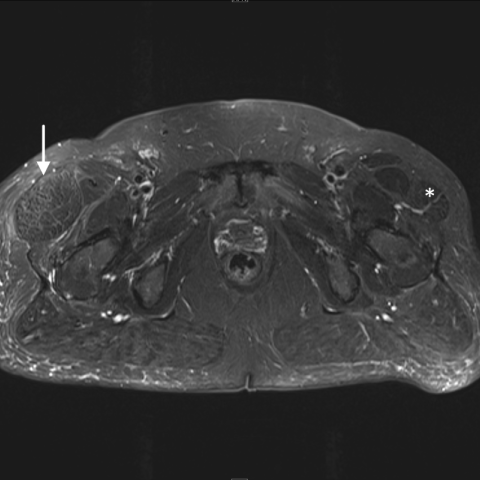
On MRI, gross asymmetry is seen in the tensor fascia latae musculature. The right tensor fascia latae is markedly hypertrophic in comparison with the contralateral side, measuring 61 mm vs 34 mm in diameter in the axial plane (Figures 1a and 1b).
Tendinopathy of the right gluteus medius and minimus is best visualised in the proton density (PD) fat sat sequence, in which a high signal is seen, corresponding to the insertion in the greater trochanter (Figures 2a, 2b, and 2c).
No histopathological samples were taken based on benign characteristics on imaging.
Discussion
Background
Tensor fascia latae pseudotumours are a benign compensatory reaction to the loss of function in the lateral hip abductors [1,3]. A similar presentation can be seen in patients suffering from lumbosacral radiculopathy [2].
The tensor fascia latae plays a supporting and stabilising role in the hip joint, as well as aiding in external rotation. The tensor fascia latae is part of the main group of hip joint abductors, together with the gluteus medius and minimus, having the capacity to compensate for loss of function in the main abductors [1,4].
Clinical Perspective
A thorough physical examination, correlated with the clinical findings, is crucial in cases where a palpable tumour and pain arise without a history of trauma.
In this patient’s case, the palpable mass was identified as compensatory hypertrophy of the tensor fascia latae, secondary to underlying tendinopathy of the hip abductors. An astute clinician can thus guide the diagnostic process towards the correct conclusion, avoiding unnecessary alarm regarding malignancy. This approach spares the patient unnecessary distress and the potential risks associated with unwarranted biopsies or surgical interventions [5].
Imaging Perspective
Soft tissue differentiation and proper visualisation of tendinopathy are most optimally seen with magnetic resonance imaging (MRI), as is shown in this case. Ultrasound as a modality can also be used for the direct visualisation of tendinopathy, with the biggest limitation being the experience level of the examiner. It is also possible to utilise computed tomography (CT) imaging, though somewhat suboptimally, as CT does not allow for direct visualisation of tendinopathy, but rather via indirect signs such as structural changes over time [5].
Take Home Message
As presented in this case, the diagnosis of tensor fascia lata pseudotumour, caused by chronic tendinopathy of gluteal abductors can be confirmed with available diagnostic imaging and physical examination.
A careful physical examination and referral to the right imaging modality made it possible to confirm the diagnosis quickly and without the need for invasive procedures. This allowed treatment to begin promptly, helping to reduce the patient’s stress. Due to the severity of the tendinopathy, surgical tendon re-insertion was performed, and the patient is now following a physiotherapy programme.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Hypertrophy of the right tensor fascia latae (pseudotumour)
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
MRI

Proton density (PD) fat sat



Medical Analysis Report
1. Imaging Findings
MRI examination of the hip in this case shows:
- There is a localized thickening and signal change in the muscle tissue on the lateral side of the right hip (lateral greater trochanter area), appearing as a bulging of the muscle structure. On T1- and T2-weighted images, the signal is similar to or slightly higher than that of normal muscle.
- Changes are observed near the tendons of the gluteus medius and minimus, with some structures displaying abnormal signals, suggesting tendon degeneration or inflammatory lesions (i.e., abductor tendon pathology).
- No obvious bony destruction or local soft tissue tumor is detected, and there is no clear sign of fracture.
- No significant abnormalities are found in the knee joint.
The overall imaging findings indicate soft tissue thickening in the lateral aspect of the right hip, consistent with a “pseudotumor” appearance, along with certain pathological features affecting the abductor tendons.
2. Possible Diagnoses
- Gluteus Medius/Minimus Tendon Lesions (tendinopathy, partial tear, or chronic degeneration): The pain and peri-acetabular soft tissue changes in this region often stem from damage to the gluteal tendons. Given the patient’s age and the prolonged duration of symptoms, as well as MRI findings of abnormal tendon signals, this is a primary consideration.
- Compensatory Hypertrophy of Hip Musculature (Tensor Fascia Latae Pseudotumor): When the main abductor muscles (gluteus medius, gluteus minimus) are compromised or injured, the tensor fascia latae may develop compensatory thickening or enlargement, resembling a soft tissue tumor.
- Other Soft Tissue Masses: Although there are no imaging features indicative of malignancy, differential diagnoses should include bursitis, lipoma, sarcoma, and other potential conditions. However, current imaging characteristics and clinical presentation do not support a malignant tumor.
3. Final Diagnosis
Considering the patient’s age, duration of symptoms, clinical examination (palpable lateral mass), and MRI findings, the most likely diagnosis is:
Tensor Fascia Latae Pseudotumor, secondary to chronic pathology of the gluteus medius and minimus tendons.
This diagnosis aligns with the absence of clear malignant features, the presence of local abductor tendon abnormalities, and the compensatory hypertrophy of the tensor fascia latae that presents as a “pseudotumor.”
4. Treatment and Rehabilitation Plan
4.1 Treatment Options
- Conservative Treatment: For early-stage or mild symptoms, prioritize physical therapy (such as ultrasound, shock wave therapy), oral or locally injected anti-inflammatory analgesics, and local cold or heat therapy to alleviate pain and inflammation.
- Surgical Treatment: For severe symptoms, inadequate response to conservative care, or significant tendon damage, surgical repair and reconstruction may be considered. This can include repair or reattachment for severely damaged tendons. Hypertrophy of the tensor fascia latae itself does not necessarily require resection; managing the primary abductor tendon pathology is crucial.
4.2 Rehabilitation Plan
Following surgery or conservative treatment, the following rehabilitation exercises and exercise prescriptions are recommended:
- Early Postoperative Phase (Weeks 1-2):
- Avoid or limit weight-bearing on the affected limb; partial weight-bearing with assistive devices (e.g., crutches) if necessary.
- Engage in small-range active and passive joint motion exercises to maintain hip joint mobility and prevent stiffness.
- Intermediate Functional Recovery (Weeks 3-6):
- Gradually increase hip flexibility training, such as supine leg raises, gentle hip abduction and adduction with light resistance, ensuring slow and controlled movements.
- Reduce reliance on assistive devices as tolerated, progressing toward full weight-bearing ambulation, while avoiding overuse and excessive pain.
- Late Strengthening Phase (6 weeks and beyond):
- Increase resistance exercises, such as using elastic bands or light weights to strengthen the gluteus medius, gluteus minimus, and tensor fascia latae for improved power and coordination.
- Gradually introduce closed-chain exercises for the lower limbs (e.g., partial squats or lunges) and moderate-intensity aerobic activities (e.g., cycling, swimming) to enhance muscular endurance.
The above regimen should follow the FITT-VP principles (Frequency, Intensity, Time, Type, Volume, and Progression) and be individualized:
- Exercise 3-5 times per week, ensuring no significant fatigue or pain before continuing or slightly increasing intensity.
- Progress intensity gradually from low to moderate, avoiding a sudden large load.
- Start each session at about 15-20 minutes and extend to 30 minutes or more as tolerated, with adequate warm-up and cool-down.
- Select appropriate types of weight-bearing and aerobic exercises, taking care to maintain proper posture to protect the hip joint.
- Adjust exercise type and intensity based on progress to prevent re-injury.
Patients with osteoporosis, cardiopulmonary limitations, or other comorbidities should exercise under the supervision of healthcare professionals to ensure safety.
Disclaimer: This report is a reference analysis based on the provided imaging data and medical history. It cannot replace an in-person consultation or professional medical advice. If you have any questions or if your condition changes, please seek medical attention promptly and follow professional instructions.
Human Doctor Final Diagnosis
Hypertrophy of the right tensor fascia latae (pseudotumour)