CT features of intraosseous lipoma of the calcaneum



Clinical History
A 30-year-old male patient presented with pain in right heel region for the past 3 months. He was referred for CT to evaluate a possible lytic lesion within calcaneum detected on plain radiography. However, the patient was not able to present he radiographs for documentation at the time of scan.
Imaging Findings
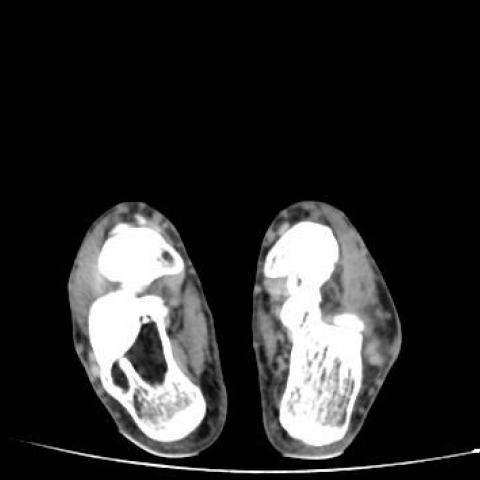
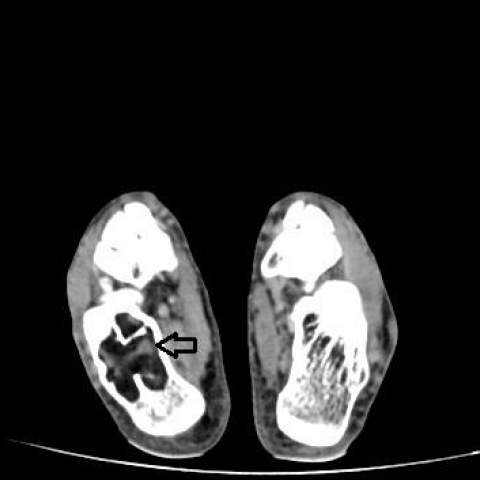
A relatively well-defined lytic lesion was seen involving the right calcaneum. On the bone window images this lesion showed a few partial bony septae/thickned trabeculae with suggestion of subtle hyperdense areas within. Mild bony expansion was also seen. Soft tissue window images revealed predominant attenuation similar to subcutaneous fat in the periphery of the lesion with central hyperdense/calcific areas confirming a diagnosis of an intraosseous lipoma with areas of fat necrosis. No pathological fractures were seen involving the lesion.
Discussion
Intraosseous lipomas (IL) are rare lesions constituting about 0.1% of bone tumours. They are commonly located in the proximal femur and calcaneum but can occur in other locations including pelvic bones and ribs [1, 2]. Although these lesions may be detected incidentally, up to 66% of patient report pain. Expansile bony remodelling and ischaemic changes have been postulated as probable causes for pain [2].
Based on radiological and pathological features Milgram classified IL into three stages [3].
Stage 1 – composed entirely of viable fat cells.
Stage 2 – composed of viable fat cells with interspersed areas of fat necrosis and calcification.
Stage 3 – composed of a large proportion of necrotic fat, calcification and cystic transformation.
The imaging appearance of IL varies depending on the stage of the lesion. Stage 1 lesions appear as well-defined lytic lesions with or without mild expansion on radiography and may mimic other lesions. CT and MRI are equally effective in demonstrating fat content within the lesion. CT demonstrates an intramedullary lesion with attenuation values ranging from – 60 to – 100 HU similar to subcutaneous fat. Attenuation values are usually slightly lower than normal marrow fat due to presence of cellular elements in yellow marrow. MRI classically shows T1 hyperintense signal with signal suppression on fat saturation sequences. Like CT the T1 signal of IL is slightly higher than marrow due to cellular elements in yellow marrow. Thickened trabecular ridges may be seen within the periphery of the lesion and are well demonstrated on CT [1, 2].
A well-defined lytic lesion in calcaneum with central calcification is pathognomonic of stage 2 IL. Calcification within IL may, however, add to confusion in other bones. Stage 2 lesions show fat attenuation with internal hyperdense areas and calcification on CT. Ischaemic changes within the lesion are thought to cause fat necrosis which appear hyperdense and may undergo calcification. The hyperdense areas may be subtle and may not be visualised on plain radiography. CT is the best modality to visualise these subtle areas. On MRI these lesions shows fat signal with internal hypointense areas corresponding to fat necrosis/calcification. Stage 3 lesions show varying degrees of calcification and cystic degeneration giving a confusing appearance on radiography. Even though cystic areas may predominate, identification of a peripheral rim of fat on CT/MRI aids in diagnosis. IL usually does not require treatment, but curettage and bone grafting may be done for symptomatic lesions [1, 2].
Differential Diagnosis List
Final Diagnosis
Intraosseous lipoma within the right calcaneum (Milgram's stage 2).
Liscense
Figures
CT foot - Bone window



CT foot - Soft tissue window

Medical Imaging Report
I. Imaging Findings
This case involves a 30-year-old male patient complaining of right heel pain for 3 months. Based on the CT images, the following findings are noted:
- A lytic lesion with a well-defined border is observed within the right calcaneus, with possible thinning and remodeling of the local cortical bone.
- The lesion exhibits a negative density, similar to fat density (approximately -60 to -100 HU), suggesting the presence of fatty components.
- Local areas of high density or calcification are visible, possibly indicating necrosis or fat calcification.
- No obvious swelling or mass is noted in the adjacent soft tissues, and there is no significant destruction of the articular surface.
II. Potential Diagnoses
Based on the above imaging findings, as well as the patient’s age and clinical symptoms, the following diagnoses or differential diagnoses are considered:
- Intraosseous Lipoma: Commonly found in the calcaneus, proximal femur, and other sites; imaging often shows fatty density or signal. If there is local calcification or necrosis, it may correspond to Milgram classification stage II or III.
- Simple Bone Cyst: Also common in younger patients. However, on CT it typically shows fluid density rather than fat density, making it less likely in this scenario.
- Aneurysmal Bone Cyst: Often presents as an expansile lytic lesion with septations and hemorrhagic components; fatty density is not typical.
- Chondroma or Cartilage-Origin Tumor: May show calcifications in cartilage (ring-like or punctate), but adjacent fatty components are not commonly seen.
III. Final Diagnosis
Taking into account the patient’s age, clinical symptoms (intermittent pain), and the CT findings of clear fat density with local calcification, the most likely diagnosis is:
- Intraosseous Lipoma (Milgram Classification Stage II)
If further confirmation of the pathological nature is required, MRI or biopsy may be considered. However, for typical imaging findings, clinical correlation often suffices for diagnostic judgment.
IV. Treatment and Rehabilitation Plan
An intraosseous lipoma is typically a benign lesion. If the lesion is small and symptoms are mild, conservative observation is an option; for symptomatic cases or those with structural risks, surgical intervention can be considered.
- Conservative Treatment: Regular follow-up imaging to monitor changes in the lesion and clinical symptoms.
- Surgical Treatment: If pain is significant or the lesion impacts function, curettage and bone grafting may be performed. In some cases, filling the cavity with graft material can alleviate pain and reduce the risk of pathological fracture.
Rehabilitation/Exercise Prescription Recommendations:
- Postoperative or Conservative Observation: Low- or non-weight-bearing exercises such as aquatic therapy or gentle range-of-motion activities are advisable.
- Gradual FITT-VP Principle:
- Frequency: 3-4 times per week, adjusted based on symptoms.
- Intensity: Begin with low intensity (e.g., stationary cycling, walking in water), increasing resistance or duration gradually.
- Time: 20-30 minutes per session, extending as pain and tolerance permit.
- Type: Choose exercises that place minimal stress on the heel, such as swimming or cycling, to reduce calcaneal load.
- Volume/Progression: As symptoms improve, gradually introduce weight-bearing exercises. Transition from walking with crutches to routine walking, and eventually to light jogging or other functional training.
- Individual Adjustments: Decrease intensity or frequency if heel pain or other discomfort occurs. Patients with lower bone density should take extra caution to avoid potential injury during weight-bearing activities.
V. Disclaimer
This report is based on the currently available imaging and information for reference only and does not replace an in-person clinical diagnosis or treatment recommendation. If you have any concerns or your symptoms worsen, please seek prompt medical attention and follow the advice of a specialist.
Human Doctor Final Diagnosis
Intraosseous lipoma within the right calcaneum (Milgram's stage 2).