


A 33-year-old man presented with swelling and pain in the right scapular region, especially with motion, accompanied by a snapping feeling of the right shoulder.
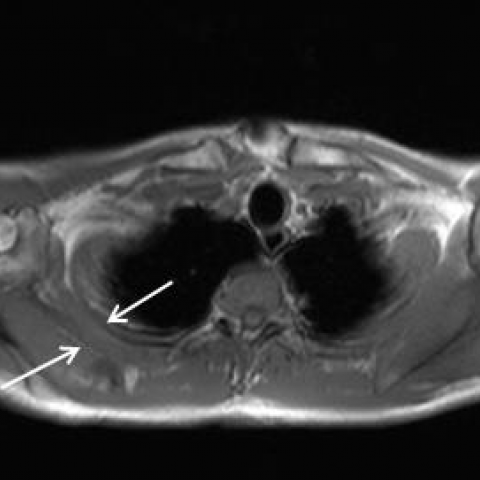
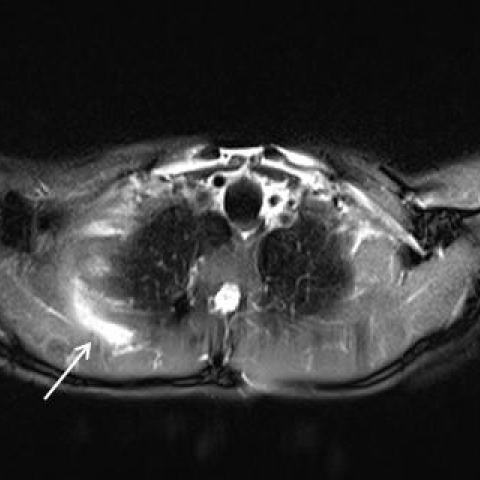
CT examination (not shown) did not reveal any bony abnormalities at the thoracic cage or scapula. Magnetic resonance imaging (MRI) was performed and showed a soft tissue mass located between the right serratus anterior muscle and subscapularis muscle. The mass had a homogeneous isointense signal intensity (compared to muscle) on T1 weighted imaging (T1WI) (Fig. 1) and high signal intensity on T2 weighted-imaging (T2WI) (Fig. 2). There was a moderate peripheral enhancement after administration of intravenous contrast medium (Fig. 3).
Fig. 1: Axial T1-weighted MR image shows a homogeneous isointense mass located between the right serratus anterior muscle and subscapularis muscle.
Fig. 2: Axial (A) and sagittal (B) T2-weighted MR images with fat suppression show a high signal intensity in this lesion.
Fig. 3: Axial T1-weighted image (fs) after intravenous Gadolinium contrast administration shows a moderate peripheral enhancement of the lesion.
Background: There are four types of bursa: adventitious, subcutaneous, synovial, and sub-muscular. Among these, only adventitious is non-native. When any surface of the body is subjected to repeated stress or constant friction, an adventitious bursa may develop under it. Two major (or anatomic) bursae and four minor (or adventitious) bursae have been described in the scapulothoracic articulation, the latter one arising as a response to abnormal biomechanics of the scapulothoracic articulation [1,2]. Two adventitious bursae have been described as lying at the superomedial angle of the scapula. A third site is at the inferior angle of the scapula. Finally, the fourth site of pathology, the trapezoid bursa, is found over the triangular surface at the medial base of the spine of the scapula under the trapezius muscle [2,3]. These bursae can become inflamed secondary to trauma or overuse owing to sports activities or work.
Clinical perspective: Scapulothoracic bursitis can be a cause of significant pain and limited mobility of the shoulder girdle region. It can be suspected clinically in patients who have pain in the scapular region with motion, occasionally accompanied by a grinding or snapping noise (crepitus) [4].
Imaging perspective: Although ultrasound is often the first-line modality performed for evaluating patients presenting with a scapular mass, MRI is the modality of choice to further characterize the lesion. MRI is especially helpful in identifying the size and location of an inflamed bursa. It usually has homogeneous decreased signal intensity on T1WI and a homogeneous bright signal intensity on T2WI. The signal intensity on T1WI can be brighter due to rich protein content [5]. MRI is also good for recognizing haemorrhagic findings in the bursa. Gadolinium administration is not always necessary if the cystic nature of the mass is obvious in pre-contrast MR studies [6]. The bursal wall may enhance due to increased vascularity. Sometimes a fluid-fluid level is revealed in the bursa [5,6]. CT may be valuable to demonstrate associated or underlying bony abnormalities, e.g. exostosis.
Outcome: The initial treatment of scapulothoracic bursitis should be conservative. Local sterile injection of corticosteroids and anaesthetics is also a viable option. Most patients improve with nonoperative measures, but for patients for whom nonoperative measures fail, surgery may be beneficial [2].
Conclusion: Scapulothoracic bursitis has typical clinical and MR features. MR findings include a cystic mass without a solid portion, situated in the subscapular region. MRI is useful to differentiate a distended bursa from neoplasm.
Scapulothoracic bursitis


Based on the provided MRI images, a cystic lesion signal is observed near the medial gliding surface of the right scapular region (the scapulothoracic joint surface). On T1-weighted images, the signal appears slightly low or moderate, whereas on T2-weighted or fat-suppressed sequences, the lesion shows high signal intensity, indicative of fluid content or inflammatory exudation. The lesion has relatively well-defined margins, with no obvious solid soft tissue component. No notable bony destruction or mass effect is seen in the surrounding scapula or adjacent soft tissue structures.
Considering the patient’s age (33-year-old male), repeated scapular region pain with characteristic clicking sensation during movement, and an MRI finding of a cystic lesion between the scapula and thoracic wall, the most likely diagnosis is: Scapulothoracic Bursitis.
If uncertainty remains, further evaluation with ultrasound or aspiration of the bursa could be performed to confirm the pathology. Based on current information, the diagnosis is relatively clear.
Under strict sterile conditions, consider injecting corticosteroids and local anesthetics into the bursa to reduce inflammation and relieve pain. This method is effective for patients with severe symptoms that affect daily activities.
For recurrent cases or those unresponsive to conservative treatment, surgical debridement or bursectomy may be performed. Postoperative shoulder rehabilitation and functional training are still required.
Disclaimer: This report is for medical reference only and does not serve as a final diagnosis or treatment recommendation. It is not a substitute for an in-person consultation or professional medical advice. If needed, please consult a relevant specialist.
Scapulothoracic bursitis