Desmoplastic fibroma of the femur


Clinical History
The patient is a 21-year-old woman who presented with persistent left knee problems with flexion-extension and going up stairs after a fall on the left knee 4 months earlier. Radiographs were taken and showed a lesion in the distal left femur. Additionally, an MR examination was performed for further evaluation.
Imaging Findings
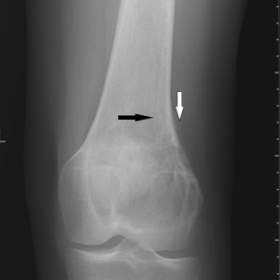
Radiographs showed a metaepiphyseal osteolytic lesion in the distal left femur with partial ill-defined outline. There was cortical breakthrough posteriorly with periostal reaction and associated soft-tissue mass.
On MR images, the tumour showed a rather homogeneous signal intensity iso-intense to muscle on T1-weighted images. Sagittal TIR images showed an inhomogeneous mass in the distal left femur containing several remarkably low signal intensity areas. There was cortical destruction of the distal left femur posteriorly with the mass extending into the adjacent soft tissues mainly periostally contained. Gadolinium-enhanced T1-weighted MR images demonstrated inhomogeneous enhancement.
Discussion
Desmoplastic fibroma (DF) is a rare benign primary bone tumour and is thought to be the intra-osseous counterpart to soft tissue fibromatoses, also known as desmoid tumour. The clinical presentation is nonspecific. The commonest presenting symptoms are pain, swelling or a palpable mass. However, some patients are asymptomatic and the lesion may be detected as an incidental finding on imaging taken for other reasons.
It can affect almost any bone but DF is most often found in the mandible, the femur, the pelvic bones, the radius and the tibia [1]. The mean age of the patients with DF at the time of diagnosis is reported to be 23 years [1], while the issue of sex predilection remains unclear. The tumour is usually found in the metaphysis or metadiaphysis, although it can extend into the epiphysis in adults after closure of the growth plate.
On radiographs, DF appears as a non-mineralized osteolytic lesion. In most cases, the lesion is well-defined with variably expressed marginal sclerosis. Periosteal reaction is exceptional but cortical thinning is often present and in fewer cases cortical breakthrough can be seen with extension into the adjacent soft tissues. Such destructive pattern with soft tissue invasion may mimic a malignant bone tumour.
On MR, T1W sequences show signal intensities within the lesion that are iso- to hypointense to adjacent normal muscles while T2W sequences demonstrate large areas of low to intermediate signal intensities compared to normal muscles [2]. Being histologically similar to the soft tissue desmoid tumour, these areas of low signal intensity on T2W images in DF may be explained by the relative low cellularity and the presence of dense fibrous matrix [4]. After intravenous gadolinium contrast administration, somewhat heterogeneous enhancement of the lesion is seen [2, 3].
The radiographic differential diagnosis of desmoplastic fibroma is very broad.
However, few bone tumours display features of a predominant osteolytic lesion with prominent T2 shortening not corresponding to calcifications on MR images, permitting to include desmoplastic fibroma in a relatively short differential diagnosis list.
DF behaves in a locally aggressive manner without capacity to metastasize.
The preferred therapy is en bloc resection since curettage alone has a higher rate of recurrence. However, when resection is not possible, curettage and grafting may be an adequate treatment modality with close follow-up.
Differential Diagnosis List
Final Diagnosis
Desmoplastic fibroma of the femur
Liscense
Figures
Anteroposterior radiograph of the left knee

Lateral radiograph of the left knee

Sagittal TIR MR image of the distal left femur

Sagittal T1-weighted MR image of the distal left femur

Axial gadolinium-enhanced T1-weighted MR image

1. Imaging Findings
Based on the provided X-ray and MRI images, the lesion is located in the distal left femur, adjacent to the knee. On X-ray, it appears as a relatively well-defined lytic lesion, with thinning of the cortical bone; in some regions there is mild sclerosis, potentially accompanied by slight soft tissue swelling. On MRI T1 sequences, the lesion’s signal is similar or slightly lower than muscle, while on T2 it exhibits predominantly low to intermediate signal intensity, suggesting a rich fibrous component. The lesion demonstrates heterogeneous enhancement overall, with a relatively well-defined margin but some features of local aggressiveness.
2. Potential Diagnoses
- Sclerotic (fibrous) bone lesion: Conditions such as fibrous dysplasia of bone, fibroma, or fibrosarcoma, which often present as lytic or mixed density lesions and may contain abundant fibrous tissue. The signal typically appears low to intermediate intensity.
- Giant cell tumor (GCT): Commonly located in the epiphysis/metaphysis of long bones around the knee, with lytic destruction and relatively well-defined margins. However, on T2 sequences it often shows higher signal intensity, and it usually occurs in people aged 20–40, so it still remains a consideration.
- Osteochondroma or chondrosarcoma: Usually visible as cartilaginous calcification or ring-like calcification on imaging, with generally higher T2 signal, which differs somewhat from this case’s imaging characteristics.
- Fibrous dysplasia: May present with a “ground-glass” density; on MRI, the signals can be variable but often appear mixed. A definitive diagnosis typically requires histopathological correlation.
Overall, considering the lytic destruction, fibrous signal characteristics, and the patient’s younger age with persistent clinical symptoms, a fibrous lesion of benign nature but with aggressive potential must be highly suspected.
3. Final Diagnosis
Taking into account the patient’s age, progressively worsening knee symptoms, the radiolucent lesion on imaging, and the low to intermediate T2 signals, the most likely diagnosis is: Desmoplastic Fibroma (DF). Although benign, it has locally aggressive behavior, so further pathological biopsy or intraoperative tissue examination is often necessary to confirm.
4. Treatment Plan and Rehabilitation
4.1 Treatment Strategy
- Surgical Treatment:
- Curettage and bone grafting or bone transplantation: This may be considered if the lesion is smaller or cannot be completely resected, but vigilant monitoring is required due to the risk of recurrence.
- En bloc resection: If feasible, complete resection of the lesion followed by reconstruction is the main method to reduce recurrence rate, possibly with internal fixation and functional reconstruction post-surgery as needed.
- Regular Follow-up: Especially after curettage, close monitoring for local recurrence is necessary, with periodic MRI or CT scans as indicated.
- Other Treatments: Since it generally lacks metastatic potential, routine radiotherapy or chemotherapy is not required. If surgical resection poses significant challenges or if special circumstances arise, multidisciplinary discussions may be necessary for any adjunctive therapy.
4.2 Rehabilitation and Exercise Prescription
Because this lesion can decrease bone support capacity and cause local pain, rehabilitation must be gradual and tailored:
- Early Phase (post-surgery or during conservative therapy)
- Focus on reducing weight-bearing and maintaining joint range of motion. Partial weight-bearing with a brace or assistive device (crutch) may be used.
- Joint ROM exercises: daily passive flexion and extension of the knee to prevent contracture.
- Isometric muscle-strengthening: for instance, isometric contractions of the quadriceps and the hamstrings.
- Intermediate Phase (after bone healing or lesion stabilization)
- Appropriately increase weight-bearing exercises on the lower limb, monitoring for pain or swelling.
- Water-based walking or simple squatting exercises can be implemented to reduce joint stress while building muscle strength and joint stability.
- Gradually increase repetition and duration, following the FITT-VP principle (Frequency, Intensity, Time, Type, Volume, Progression).
- Later Phase (functional reconstruction stage)
- When bone healing is sufficient, stationary or recumbent cycling can be added to improve knee ROM and cardiovascular endurance.
- Gradually return to low-impact exercises such as jogging on level ground or using an elliptical trainer, while monitoring for pain or recurring functional limitations.
- Combine with core strength training to enhance lower limb muscle coordination and prevent re-injury.
Throughout rehabilitation, it is crucial to monitor for knee swelling, pain, or restricted movement. If significant discomfort occurs, please consult a physician or rehabilitation specialist promptly.
5. Disclaimer
This report is based solely on the provided images and brief clinical information. It serves as a reference and cannot substitute an in-person consultation or professional medical opinion. For specific treatment plans or risk assessments, please consult a specialist to obtain more accurate and individualized guidance.
Human Doctor Final Diagnosis
Desmoplastic fibroma of the femur