Munchmeyer's Disease



Clinical History
A 10-year-old female presented with the chief complaint of progressive inability to open the mouth since the past year and multiple firm round swellings on the vertebral region, right scapula and right occipital region of the skull. She had laterally deviated short first toes of both feet.
Imaging Findings
1. PA chest showing extensive focal and cord-like ossification of muscles and soft tissue of back, chest, abdomen and visualised right arm giving pattern of branching tree.
2. AP radiograph of both feet showing microdactyly of the great toes and bilateral hallux valgus.
3. Lateral view of thorax and abdomen showing cord-like ossifications of muscles of back
4. Axial CT images of thorax showing ossification of back, chest muscles.
5. 3D Coronal CT image showing posterior view of trunk and neck exhibiting excellent demonstration of soft tissue and muscle ossifications mimicking ‘tree branching pattern’.
6. 3D Coronal CT image showing anterior view of trunk and neck exhibiting excellent demonstration of soft tissue and muscle ossifications mimicking ‘tree branching pattern’.
Discussion
Munchmeyer's disease or Fibrodysplasia ossificans progressive (FOP) is a rare autosomal dominant disease [1]. It is also known as myositis ossificans progressive or stone man disease [2]. It was first described by Patin [3]. The worldwide prevalence of FOP is approximately 1 in 2,000,000 [4]. It is most commonly seen between birth and 10 years of age. The mean age of occurrence is three years. Pathologically it is characterized by progressive replacement of muscles, tendons, ligaments, fascia and aponeurosis by bone, leading to progressive stiffness of the adjacent joints. The progressive replacement of the chest wall may lead to pneumonia and death [5]. FOP is characterized by two cardinal features: a)heterotopic progressive osteogenesis, b) congenital abnormalities of the great toes [2]. However it is particularly disabling in children. The most characteristic deformity is microdactyly of both halluces due to a single phalanx in valgus position [6, 7]. This characteristic feature is found in our case also. The patients affected by FOP are usually confined to bed by the age of 30. FOP primarily involves the neck (50%), dorsal paraspinal region (30%), head (10%) or limbs (10%). The 70% of FOP patients develop temperomandibular joint ankylosis [8]. The ectopic ossification is a hallmark sign of FOP. It can occur during the lifespan of a patient but most commonly it is found between 3 to 5 years of age [8, 9]. Radiologically, myossitis ossificans progressiva can be identified approximately two to four weeks after the onset of the process. In FOP, computed tomography can be used to delineate the central radiolucency encompassed by peripheral density [10]. The radiographs may aid in documenting minor osseous dysmorphism. Bone scintigraphy with 99mTc-MDP demonstrates early heterotopic ossification and helps in assessment of the extent and progression of the FOP [7]. The effective treatment for FOP is still unknown. FOP is managed conservatively by avoiding conditions potentially provocative of abnormal ossification. However administration of calcium chelators such as sodium etidronate and corticosteroids reduces the progress of the disease [10].
Differential Diagnosis List
Final Diagnosis
Munchmeyer's disease or Fibrodysplasia ossificans progressive
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Axial CT image

Axial CT image of thorax
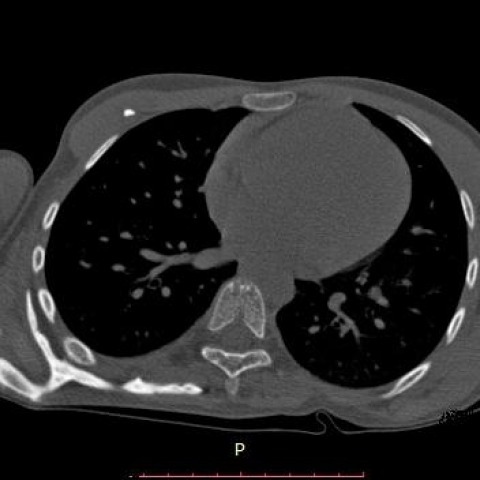
Axial CT image

3D CT image (Coronal section)

3D CT image(Coronal)

Panoramic Radiograph

Postero-Anterior view(PA) Chest

Antero-posterior view(AP) of feet

Lateral view of thorax and abdomen

Medical Imaging Analysis Report
I. Radiological Findings
Based on the provided chest CT, spinal and limb X-rays, as well as cranial imaging (including panoramic radiography of the maxillofacial region), the following main characteristics are observed:
- Thoracic, dorsal, and paraspinal regions: CT and 3D reconstruction reveal cord-like or lump-like areas of increased density within the vertebral bodies and paravertebral muscular regions, resembling bone tissue and suggesting significant heterotopic ossification. In some areas between the ribs and vertebral bodies, exostosis can also be seen, leading to restriction of the thoracic cage.
- Cervical region and skull: Sclerotic changes or bone-like proliferations are observed in the right occipital region of the posterior skull; imaging of the mandible suggests a marked reduction in the range of motion of the temporomandibular joint, possibly indicating heterotopic calcification in the joint or surrounding soft tissues.
- Limbs: Bilateral foot X-rays show that the first toe (hallux) is significantly shortened and deviated laterally, with only a single (or fused) phalanx remaining, consistent with the typical congenital anomaly of the first toe (shortened and valgus).
- Other soft tissue ossifications: Multiple high-density lesions with bone-like density are seen in the scapular region, paraspinal muscles, and soft tissues of the back. Their well-defined margins are consistent with imaging findings of heterotopic ossification.
II. Potential Diagnoses
- Fibrodysplasia Ossificans Progressiva (FOP) - This disease is an autosomal dominant genetic disorder characterized by progressive ossification of soft tissues such as muscles, fascia, and ligaments. - The classic “stone man syndrome” shows patchy or cord-like ossifications within muscles or fascia on imaging. - Congenital malformation of the great toe is a key diagnostic feature. - Imaging findings show a high degree of consistency with clinical history (difficulty opening the mouth, multiple round or cord-like ossifications), suggesting this diagnosis.
- Other rare heterotopic ossification disorders - For instance, Progressive Osseous Heteroplasia, etc., but most do not present the typical first-toe malformation.
- Recurrent muscle or fascial calcification/ossification - Such as post-traumatic or post-infectious calcifications, usually associated with a history of trauma and lacking the characteristic bilateral toe deformities.
III. Final Diagnosis
Combining the onset at 10 years of age, progressive difficulty opening the mouth, abnormal soft tissue ossifications in the back and head, and bilateral congenital malformation of the first toe (short and valgus), the most fitting diagnosis is:
Fibrodysplasia Ossificans Progressiva (FOP).
This disease has highly specific clinical and radiological features, including congenital hallux deformities and progressive heterotopic ossification within soft tissues.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Conservative management: Currently, there is no curative treatment. Efforts should be made to avoid trauma, intramuscular injections, and unnecessary surgical procedures to prevent new areas of ossification.
- Pharmacological intervention: During active inflammatory periods or early in the formation of new ossification lesions, a short course of corticosteroids (e.g., prednisone) may help reduce acute inflammation. Bisphosphonates (such as etidronate) or other calcification inhibitors may also be used to slow the progression of ossification.
- Supportive therapy: For functional impairments resulting from established heterotopic ossifications, physical therapy and orthotic support can be provided.
2. Rehabilitation and Exercise Prescription
Because FOP patients are prone to further ossification in joints and soft tissues, any inappropriate or forceful therapeutic measures may exacerbate ossification. Rehabilitation should be carefully managed, focusing on safety and a gradual approach:
- Frequency: Recommended 2-3 times per week, adjusted according to the patient’s tolerance and stability of the condition.
- Intensity: Emphasize mild passive or active range-of-motion exercises, avoiding pain or marked discomfort to prevent new ossification.
- Time: Each session should start with 5-10 minutes of exercises, gradually increasing to 15-20 minutes while monitoring the patient’s subjective experience.
- Type: Primarily range-of-motion maintenance exercises, gentle stretching, and mild muscle strengthening (such as low-resistance band exercises or isometric training). Strenuous or high-impact activities must be strictly avoided.
- Progression: Increase intensity and duration gradually, based on stable disease status. Monitor closely for any new heterotopic ossification or pain responses.
If the thoracic cage or cervical spine is involved, breathing exercises (such as deep breathing) should be performed with caution to avoid excessive stretching of the chest and back muscles.
V. Disclaimer
The above report is a reference-based medical analysis based on existing information and does not replace in-person consultation or professional medical advice. If you have any questions or changes in symptoms, please consult a physician promptly.
Human Doctor Final Diagnosis
Munchmeyer's disease or Fibrodysplasia ossificans progressive