Sacral fractures: How should we classify them?



Clinical History
86-year-old patient who reported 5 days of lumbosacral pain after a fall on a bus.
Imaging Findings
X-RAY
Sacral fractures can often be difficult to visualize on an AP radiograph because of the inclination angle of the sacrum.
CT:
Multiple sacral fractures are observed. We will classify them following the two main classifications known for sacral fractures without other pelvic ring fractures:
DENIS CLASSIFICATION (Key point: to assess possible neurologic damage)
- Fig.1: ZONE 1 FRACTURES
These fractures are lateral to the sacral foramina.
- Fig.2 and Fig.3: ZONE 2 FRACTURES
These fractures involve one or more of the foramina. Neurologic deficits occur in a few cases.
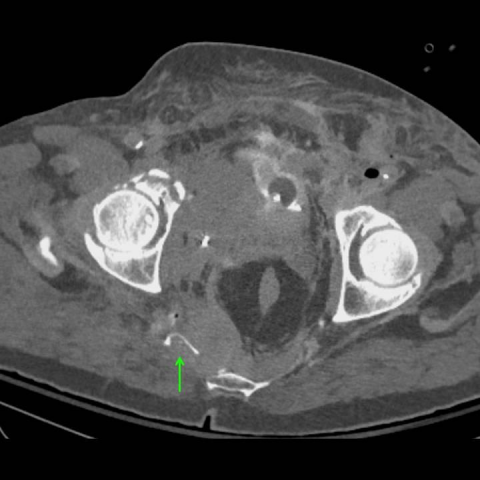
- Fig.4: ZONE 3 FRACTURE
A transverse zone 3 fracture, subtype 2 (partial anterior translation and hyperkyphotic) is observed. This kind of fractures could be caused by a direct trauma. Neurologic damage was not found in our case.
ISLER CLASSIFICATION (Key point: to assess lumbosacral stability)
Sacral fractures have caused a type A lumbosacral injury: fracture line is lateral to L5-S1 facet, no lumbosacral instability was found (Fig.5).
Discussion
A- BACKGROUND [1, 2]
- Sacral fractures most commonly occur after pelvic ring injuries.
- Sacral fractures are generally classified into three categories:
1. Those associated to pelvic ring fractures: Letournel, Tile, and AO-ASIF classification systems.
2. Those that involve the lumbosacral junction (Isler classification).
3. Those intrinsic to the sacrum (Denis classification).
- Isolated sacral fractures are typically caused by high-energy traumas. They tend to associate with vertical shear pelvic fractures and are usually unstable.
- Sacral fractures associated with lateral compression pelvic fractures are usually stable.
B - CLINICAL PERSPECTIVE
This is a case of multiple sacral fractures without other pelvic ring fractures. Accordingly, we will be using Denis classification in the first place. Second, we will use Isler classification due to lumbosacral extension of these factures.
------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------
C- DENIS CLASSIFICATION [3, 4]
(Key point: to assess possible neurologic damage)
1. Zone 1 fractures (Fig.1)
- These fractures are lateral to the sacral foramina.
Neurologic deficits are unlikely, although sciatic nerve or L5 nerve root could be damaged.
Sacral stress fractures occur in the sacral wing (zone 1).
2. Zone 2 fractures (Fig.2; Fig.3)
- These fractures involve one or more of the foramina.
Neurologic deficits occur in a few cases, presenting with unilateral lumbar or sacral radiculopathies.
- If a shear component is present, they are highly unstable.
3. Zone 3 fractures (Fig.4)
- These fractures involve the central sacral canal.
Neurologic damage is likely (sexual or sphincter dysfunction, bladder incontinence, saddle anaesthesia).
- Transverse zone 3 fractures are classified as zone 3 fractures (traverse the spinal canal). S1- S3 involvement, higher prevalence of bladder dysfunction.
Roy-Camille et al. and Strange-Vognsen and Lebech have further classified these fractures:
.
- Type 1: Simple flexion deformity of the sacrum, kyphotic angulation.
- Type 2: Partial anterior translation and hyperkyphotic (Fig.4).
- Type 3: Complete anterior translation with no fracture overlap.
- Type 4: Comminution of the S1 vertebral body caused by axial loading.
Transverse fractures have also been described based on morphology as H, U, lambda and T-shaped fractures.
------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------
D- ISLER CLASSIFICATION [4]
(key point: to assess lumbosacral stability)
It is based on the injury at the lumbosacral junction (relative to the L5-S1 facet).
-Type A- lateral to L5-S1 facet, no lumbosacral instability (Fig.5).
-Type B- through the L5-S1 facet joint.
-Type C- medial to the facet joint, crossing into the neural arch (significant instability). Bilateral type III injuries may lead to lumbosacral dissociation.
Differential Diagnosis List
Final Diagnosis
Multiple sacral fractures (without other pelvic ring fractures).
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Zone 1 fractures



Isler type A fracture

Zone 2 fractures

Zone 2 fractures


Zone 3 fracture: Transverse fracture

1. Imaging Findings
According to the provided pelvic and lumbosacral CT images, multiple fracture lines are visible in the sacrum. The specific findings are as follows:
- On axial (transverse) and coronal reconstructed images, fracture lines can be seen in both sacral ala regions, near the sacral canal, with some fracture lines passing through the areas of the sacral foramina (i.e., medial portion of the sacral ala).
- The sagittal reconstruction shows that the course of the fracture involves parts of the posterior structures of the sacral vertebral bodies, but there is no clear forward displacement or large-scale collapse.
- No obvious concomitant fractures in the pubis, ilium, or ischium were seen, indicating that the integrity of the pelvic ring appears relatively maintained.
- No significant large hematoma was observed in the surrounding soft tissues, and no evident signs of sacral nerve root compression on imaging. However, clinical neurological examination is necessary to rule out possible nerve injury.
2. Possible Diagnoses
Based on the patient’s advanced age, history of trauma (a sudden brake on a bus or a fall), and imaging findings, the following possibilities are considered:
- Traumatic Sacral Fracture (Primarily Denis Zone 2)
- The fracture mainly involves the sacral ala and the region near the sacral foramina, consistent with the typical presentation of Denis Zone 2.
- This region could be fractured due to direct impact or transmitted stress; in some patients with osteoporosis, relatively minor trauma may result in fracture.
- Sacral Insufficiency Fracture (on the background of osteoporosis)
- In elderly females with osteoporosis, low-energy injuries such as a simple fall can also lead to sacral fractures.
- However, this patient has a clear acute traumatic event, making a traumatic fracture more likely, though chronic stress or osteoporotic factors may be overlapping concerns.
- Concurrent or Potential Sacral Nerve Root Injury
- Although no obvious nerve root compression is seen on imaging, the fracture lines passing through the foramina region raise the possibility of unilateral or bilateral sacral nerve root compromise.
- Neurological examination and possibly electrophysiological evaluations are required.
3. Final Diagnosis
Considering the patient’s old age, history of falling trauma, and CT imaging showing multiple sacral fracture lines, the diagnosis most consistent with these findings is:
- Multiple traumatic sacral fractures, primarily located in Denis Zone 2, with no indication of pelvic ring fracture.
Additionally, given that the fractures involve sacral foramina and are near the sacroiliac joint and L5-S1 facet joints, Isler classification may be used for further subclassification. From the images, the fractures appear mostly lateral to or close to the facet joint area, suggesting a possible Isler Type A or Type B classification (a detailed three-dimensional reconstruction and clinical biomechanical assessment would be necessary for final confirmation).
4. Treatment Plan and Rehabilitation Strategy
4.1 Treatment Strategy Overview
- Conservative Treatment: Suitable for stable fractures with no significant displacement and mild or no neurological deficit. This includes bed rest, wearing a lumbosacral brace, analgesics, and management of osteoporosis (for example, calcium and vitamin D supplements, bisphosphonates, or calcitonin).
- Surgical Treatment: If significant fracture displacement, severe neurological symptoms, or instability (e.g., Isler Type B or C with marked facet involvement) are present, percutaneous screw fixation, sacroiliac screw fixation, or other individualized surgical interventions may be considered.
- Neurological Assessment: If any symptoms such as sensory changes, decreased muscle strength, or bowel/bladder dysfunction are noted or suspected, electrophysiologic studies and MRI may be indicated. In cases of acute nerve compression or progressively worsening neurological deficits, prompt surgical decompression is necessary.
4.2 Rehabilitation/Exercise Prescription Recommendations
Considering the patient’s advanced age, osteoporosis, and existing risk of sacral fracture, an individualized, gradual, and safety-oriented approach should be adopted:
- Early Recovery (Acute Fracture Phase: 2-4 weeks)
- Focus on protective immobilization and pain management; a lumbosacral support brace can be used depending on pain levels.
- Encourage gentle lower limb activity: ankle pumps and knee flexion/extensions in sitting or lying positions to prevent lower-limb thrombosis.
- Use assistive devices (walker or cane) for short indoor ambulation; permit mild weight bearing as tolerated, ensuring patient safety.
- Intermediate Functional Recovery (about 4-8 weeks)
- Gradually increase weight-bearing as pain allows, such as short-distance walking a few times a day (2-3 sessions of 10-15 minutes each), while avoiding prolonged standing or sitting.
- Begin core muscle strengthening exercises: supine bridge (hip lift) or simplified lumbar/back muscle training, executed gently and slowly.
- Closely monitor pain and neurological symptoms; adjust or reduce exercise if symptoms worsen.
- Late-Stage Reinforcement (about 8-12 weeks and beyond)
- Progressively resume normal daily activities; incorporate lumbar and core stabilization exercises. If conditions allow, balance training such as partial squats or use of a balance board can be introduced.
- Gradually increase walking duration and frequency; for instance, add 5-10 minutes per week, monitoring for fatigue and joint stress.
- After fracture healing is confirmed and if cardiopulmonary function permits, consider low-impact aerobic activities such as stationary cycling or swimming.
Throughout the rehabilitation process, adherence to the FITT-VP principle (Frequency, Intensity, Time, Type, Volume, Progression) and individualization is emphasized, adjusting interventions based on bone density and pain tolerance.
Disclaimer: This report is provided as a reference based on current imaging findings and the patient’s history and does not replace an in-person consultation or professional medical advice. If you have any concerns or if symptoms worsen, please seek medical attention promptly for further evaluation or treatment.
Human Doctor Final Diagnosis
Multiple sacral fractures (without other pelvic ring fractures).