Bipartite medial cuneiform: congenital variant in a patient with foot trauma. MRI findings



Clinical History
The patient presented with mid-foot medial pain, due to a blunt trauma two days earlier. He had no functional limitation and had no relevant medical history.
Imaging Findings
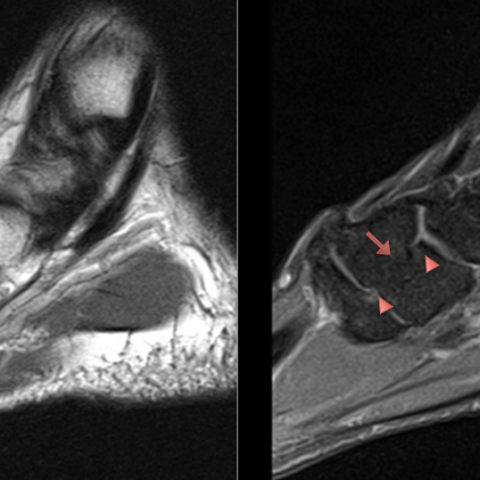
MR images showed soft tissue oedema consistent with recent trauma (fig. 1), and a complete bipartite medial cuneiform with dorsal and plantar components. Sub-cortical degenerative changes with osseous edema were observed at the plantar segment (fig. 2).
Discussion
Bipartite medial cuneiform (BMC) is a rare congenital variant at the Lisfranc joint. In humans, the incidence of this finding ranges from 0.3% to 2.4% in cadaveric studies [2, 3].
Bi-partition of the medial cuneiform is a malsegmentation defect based on the prevalence of two unfused primary ossification centres (dorsal and plantar segments) that remain apart through a fibrocartilaginous/cartilaginous synchondrosis. Normally, the medial cuneiform is formed by one ossification centre. Ossification of the medial cuneiform begins at the age of 2, in this case ensuing two fragments [2, 3].
Bipartite medial cuneiform can be assigned to one of three described morphological categories:
A. Complete bi-partition, in which the medial cuneiform is divided into two upper elements, dorsal and plantar (fig. 1).
B. Incomplete bi-partition, in which the two segments are partially fused, with clefts on the medial and lateral surfaces that demark dorsal and plantar segments (fig. 4).
C. Division of the distal articular surface only.
There is a slight predilection for males, bilaterality can be expected in 60% of the cases [4].
Diagnosis through plain radiographs can be challenging due to superimposition of osseous structures, lateral view proved to be the best perspective, moreover lateral oblique view (30 °) has been suggested to aid diagnosis [2, 4, 5]. The gap in the joint space between the ossicles of the BMC and the first ray, create a rift in “E” configuration, hence the “E sign” appreciated in a sagittal/lateral views [2-4, 6], (fig. 3). Sophisticated imaging techniques such as TC or MRI have shown great impact in high detailing this finding, with the use multiplanar reconstruction (along with 3D virtual rendering) and the possibility of depicting bone marrow oedema respectively [2-5].
BMC is vastly an asymptomatic finding, symptomatic BMC can cause midfoot chronic pain due to inflammation/disruption of fibrocartilaginous synchondrosis during high impact sporting activity, or after taking a direct blow [2-5].
The main differential diagnosis to consider is the medial cuneiform fracture, which has irregular edges, and usually splits the cuneiform vertically into an anterior and posterior fragment. Isolated medial cuneiform fractures are rare, only after a direct trauma [2-6].
When a BMC becomes symptomatic, treatment alternatives range from orthotics, immobilization, corticosteroid injections, to surgical interventions including fusion and excision of bone fragments [2-5].
Differential Diagnosis List
Final Diagnosis
BIPARTITE MEDIAL CUNEIFORM
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Complete Bipartite Medial Cuneiform

Complete Bipartite Medial Cuneiform

"E" Sign

Partial Bipartite Cuneiform
Medical Analysis Report
I. Imaging Findings
Based on the patient’s MRI examination (considering the sagittal and axial views provided), the following key features are noted:
- In the medial aspect of the tarsal bones, the cuneiform region shows a “bipartite” morphology, with the medial cuneiform separated into an upper and lower bony segment connected by fibrocartilage or cartilage, rather than a complete osseous union.
- On the sagittal view, an “E sign” (joint space shaped like the letter “E”) can be observed, suggesting a stable or semi-stable fibrocartilaginous connection between the upper and lower segments of the medial cuneiform.
- No obvious fracture line or fracture fragments; trabecular continuity is largely preserved, with mild bone marrow edema (possibly related to increased local stress and soft tissue reactions post-trauma).
- Surrounding joint structures are relatively intact, with no clear signs of tendon or ligament rupture.
II. Possible Diagnoses
- Bipartite Medial Cuneiform (BMC)
- Features: Often caused by two primary ossification centers failing to fuse, resulting in an upper and lower portion connected by fibrocartilage or cartilage. Frequently a congenital variant, usually asymptomatic; however, it may become painful if trauma or excessive loading occurs.
- Imaging Characteristics: On the sagittal view, it often presents an “E-shaped” joint space (“E sign”); the edges of the upper and lower segments are smooth and well-defined, without a clear fracture line.
- Medial Cuneiform Fracture
- Features: Typically caused by trauma, characteristically displaying irregular fracture lines and fragment displacement. Anterior-posterior separation is more common (unlike the superior-inferior segmentation seen in BMC).
- Imaging Characteristics: Fracture sites may show clear cortical discontinuity and sharper, irregular edges, often accompanied by local soft tissue swelling.
Based on the imaging findings in this case and supporting literature, congenital bipartite medial cuneiform aligns better with the observed features, especially the smooth contours of the bony segments and the notable “E sign.”
III. Final Diagnosis
Taking into account the patient’s age, symptoms (mild pain, limited but not disabling functional restriction), history of blunt trauma, imaging results, and lack of significant fracture displacement, the most likely diagnosis is: Bipartite Medial Cuneiform (BMC).
Although there is a history of trauma, the imaging does not indicate typical medial cuneiform fracture characteristics. Bipartite medial cuneiform may become symptomatic due to trauma or heavy loads, suggesting that current symptoms are more likely a post-traumatic exacerbation of a congenital BMC.
IV. Treatment Plan and Rehabilitation
Given the patient’s mild symptoms and no significant functional impairment, the following management and rehabilitation strategies are recommended:
- Conservative Treatment
- Short-term reduction of high-load or high-impact activities to avoid worsening inflammation at the cartilage junction.
- Use arch supports or custom foot orthotics to maintain proper foot alignment and reduce local stress.
- If pain is severe, under medical supervision, consider NSAIDs (non-steroidal anti-inflammatory drugs) or local corticosteroid injections to reduce inflammation.
- A short-term ankle-foot brace or elastic bandage may be used to provide stable support during the acute phase.
- Rehabilitation Training Recommendations (FITT-VP Principle)
- Frequency: 3-4 sessions of rehabilitation exercises per week are advised, allowing 1-2 days of rest between sessions for adequate recovery.
- Intensity: Begin with low-intensity exercises, such as active foot and ankle movements and light lower extremity strengthening. Avoid prolonged weight-bearing or high-impact activities.
- Time: Each session should last approximately 20-30 minutes, increasing gradually according to the patient’s tolerance.
- Type: May include seated ankle exercises (plantar flexion, dorsiflexion), foot-strengthening exercises with resistance bands (see examples below), and lower-limb core stability drills (like seated or standing balance training).
- Progression: As pain subsides and foot strength and stability improve, exercises can gradually incorporate greater weight-bearing or longer durations. Pain and discomfort should be monitored, and the training load adjusted as necessary.
- Example: Provided there is no significant pain, each session can include:
- Ankle circles: 10-15 rotations clockwise and counterclockwise
- Plantar flexion/dorsiflexion with a resistance band: 8-10 repetitions per set, for 2-3 sets
- Single-leg standing (as tolerated): maintain for 10 seconds, repeat 5-8 times, with support from a wall or stable object if needed
- Surgical Intervention
- Considered only if symptoms are recurrent or significantly affect function and conservative treatments fail (e.g., cartilage rupture or persistent pain).
- Potential procedures include fusion or excision of one fragment, but careful evaluation of local biomechanics is necessary.
Special Note: As the patient is older, bone quality (e.g., osteoporosis) should be evaluated. Gradual progression in strengthening and weight-bearing exercises is essential to avoid excessive stress concentration.
Disclaimer: This report is based solely on current examinations and available information. It does not replace in-person consultation or professional medical advice. If you have any concerns or your symptoms worsen, please seek medical attention or further evaluation promptly.
Human Doctor Final Diagnosis
BIPARTITE MEDIAL CUNEIFORM