Rice bodies associated with rheumatoid arthritis



Clinical History
A 57-year-old female patient with a history of longstanding seronegative, ANF-positive rheumatoid arthritis presents to the department of orthopedic surgery with shoulder pain.
Imaging Findings
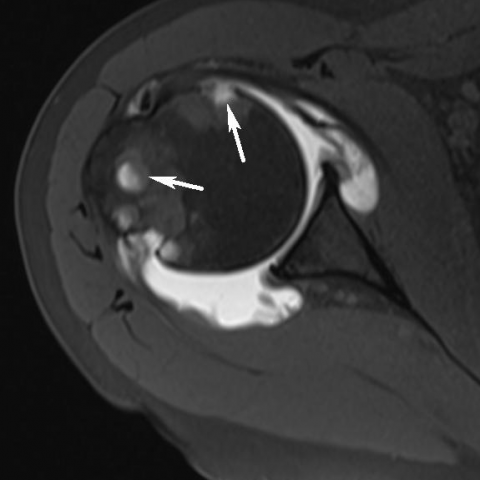
Plain radiography of the right shoulder revealed degenerative changes at the acromioclavicular joint and sclerotic delineated erosions at the humeral head (Fig. 1). Conventional Arthrography of the right shoulder showed irregular delineation of the joint capsule with multiple intra-articular filling defects and a partial articular infraspinatus tear (Fig. 2). Subsequent MR Arthrography confirmed erosions at the anatomical neck, the partial articular tear of the infraspinatus tendon and the intra-articular foci of intermediate signal on both pulse sequences, in keeping with rice bodies (Fig. 3). Plain radiographies of the hands and feet performed at a previous date showed sequelae of longstanding rheumatoid arthritis (Fig. 4).
Discussion
The term rice body was originally coined in 1895 due to its resemblance to polished grains of rice [1]. Rice bodies are considered a non-specific response to synovial inflammation, most commonly found in rheumatoid arthritis (RA) [2]. Other causes of rice body formation are tuberculous arthritis, septic arthritis and spondyloarthropathy [3, 4].
Its pathogenesis is not fully understood. Most authors believe that rice bodies result from micro-infarcts in hypertrophic synovium, leading to detachment of synovial free fragments into the joint cavity. Histologically rice bodies consist of acidophilic amorphous core surrounded by fibrin and collagen [3, 4]. They appear to be unrelated to disease activity, severity or duration [1, 2, 5, 6].
Plain radiography (CR) is usually nonspecific and adds little in the diagnosis. Although CR may show marginal erosions as a consequence of longstanding underlying joint disease in RA, direct visualisation of rice bodies, however, is impossible. Conventional arthrography may reveal multiple intra-articular filling defects. Ultrasound shows multiple hyperechoic, intra-articular loose bodies, associated with signs of arthritis including hypervascular synovial inflammation, bursitis and erosions [4]. The imaging modality of choice is MRI or MR arthrography. On MRI, rice bodies appear as multiple intra-articular foci iso- or hypointense to skeletal muscle on T1-weighted images (WI) and hypointense on T2-WI [2-5].
The differential diagnosis on imaging includes synovial chondromatosis, pigmented villonodular synovitis (PVNS) and lipoma arborescens. Synovial chondromatosis may be primary or secondary due to underlying joint disease. The signal intensity of the intra-articular loose bodies is variable according to the stage of the disease. Loose bodies may contain hyaline cartilage in the initial stage, which may later calcify or ossify. PVNS is characterised by hypointense synovial structures on both pulse sequences and shows blooming artefacts on gradient echo imaging, due to the presence of hemosiderin. In joints with a tight capsule bone erosions are often associated. Lipoma arborescens consist of a subsynovial lipomatous soft tissue proliferation which is isointense to fat on T1- and T2-WI [7].
Removal of rice bodies may correlate with clinical improvement in affected joints [1, 2]. Some authors recommend aspiration or arthroscopic lavage or surgical synovectomy as potential treatment options [1, 3, 4].
In conclusion, rice bodies are a relatively uncommon imaging finding in patients with longstanding articular disease. Meticulous analysis of the imaging findings, knowledge of underlying joint disease, such as RA, and correlation with previous imaging allows a correct diagnosis.
Differential Diagnosis List
Final Diagnosis
Rice body formation in rheumatoid arthritis.
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Anteroposterior plain radiography of the right shoulder

Shoulder arthrogram


Magnetic resonance of the right shoulder




Plain radiography of hands and feet


Medical Imaging Analysis Report
I. Imaging Findings
1. On the shoulder joint X-ray, multiple round or irregularly dense shadows can be seen within the Glenohumeral joint space. Some lesions have relatively clear margins and are scattered in distribution.
2. MRI shows multiple small entities within the joint space and synovial sacs, with signals similar to or slightly lower than muscle. In T1-weighted images, they appear as low to isointense signal, and in T2-weighted and fat-suppressed sequences, they mostly present as low signal. Partial lesions show surrounding synovial thickening and marked enhancement.
3. Local inflammatory changes are observed in the soft tissues around the shoulder joint, including synovial hypertrophy, subacromial bursa effusion, and synovial enhancement.
4. Previous X-ray images of the patient's hand and foot joints show chronic changes consistent with rheumatoid arthritis (RA), such as marginal erosions and joint space narrowing.
II. Potential Diagnoses
- Rheumatoid Arthritis (RA) with Rice Bodies Formation:
Based on the patient's long-term RA history, the presence of multiple millet-like or “rice-like” bodies within the synovium is commonly seen in chronic synovitis. Imaging characteristics show multiple low-signal bodies within the joint (especially on T2-weighted sequences), which aligns with the literature describing Rice Bodies.
- Synovial Chondromatosis:
Can present as multiple cartilaginous or calcified bodies within the joint. However, in this case, most of the small entities exhibit low signal on MRI, with no obvious calcification or ossification. Combined with the clinical background, this is less likely.
- Pigmented Villonodular Synovitis (PVNS):
Often appears as diffuse or focal synovial lesions within the joint, and MRI typically shows low signal due to hemosiderin deposition along with “blooming” artifacts. In this case, the multiple free bodies are more in line with Rice Bodies rather than typical PVNS manifestations.
- Joint Tuberculosis (or Tuberculous Synovitis):
May also present with Rice Body-like changes. However, the patient’s primary history is rheumatoid arthritis, and there is a lack of typical systemic or local tuberculous infection signs (e.g., significant night sweats, systemic wasting, characteristic joint destruction). Thus, it is not the top consideration here.
III. Final Diagnosis
Combining the long-standing RA history, shoulder pain symptoms, and imaging findings of multiple low-signal (on T2-WI) free bodies, the most likely diagnosis is:
“Rheumatoid Arthritis with Rice Bodies Formation.”
If there is still uncertainty, arthroscopy or biopsy of the synovium and loose bodies can be performed to confirm the nature of Rice Bodies.
IV. Treatment Plan and Rehabilitation
1. Conservative and Pharmacological Treatment:
- For patients with significant joint pain, use disease-modifying antirheumatic drugs (DMARDs), such as Methotrexate, and short-term corticosteroids under rheumatology specialist guidance to reduce inflammation.
- Local physical therapy and non-steroidal anti-inflammatory drugs (NSAIDs) can be used to relieve joint pain.
2. Arthroscopic Debridement or Surgical Treatment:
- For severe symptoms, recurrent effusion, or marked synovial proliferation, arthroscopic removal of Rice Bodies and synovial debridement or synovectomy can effectively alleviate symptoms and improve joint mobility.
- If there is severe structural damage to the shoulder joint, it is necessary to assess the indication for shoulder arthroplasty.
3. Rehabilitation and Exercise Prescription:
- Early Rehabilitation (Acute Phase with Uncontrolled Inflammation):
- Provide adequate rest and avoid overuse of the affected limb; local warm therapy can help improve blood supply.
- Perform low-intensity active or passive range-of-motion exercises for the shoulder, such as pendulum exercises, once or twice daily for 5-10 minutes each time. Movements should be gentle to avoid exacerbating pain.
- Intermediate Phase (Pain is Manageable, Inflammation Relatively Stable):
- Gradually increase active range of motion of the shoulder (e.g., wall-climbing exercises, forward flexion and abduction stretches) 3-4 times per week, 10-20 minutes each time.
- Under the supervision of a physical therapist, use resistance bands or light weights to strengthen the rotator cuff muscles.
- Later Phase (Functional Recovery):
- Within tolerance, add multi-angle load-bearing exercises for the shoulder, such as dumbbell abduction and external rotation, 3 times per week, 15-25 minutes each time.
- Incorporate daily functional training to enhance shoulder stability and proprioception, such as reaching overhead for objects or light wall push-ups.
- Throughout the rehabilitation process, the range of motion, pain level, and strength recovery should be regularly evaluated. Gradually increase training intensity and duration, carefully monitoring for joint inflammation or injury.
V. Disclaimer
This report is a comprehensive reference analysis based on imaging data and related medical history. It does not replace an in-person consultation or professional judgment of a clinical physician. Any treatment or rehabilitation decisions should be made in conjunction with the patient’s actual condition and under the guidance of a professional medical team.
Human Doctor Final Diagnosis
Rice body formation in rheumatoid arthritis.