Bilateral posterior shoulder dislocation with reverse Hill-Sachs lesion



Clinical History
A 49-year-old woman with a past medical history of encephalopathy presented at the emergency department after an epileptic seizure with bilateral shoulder pain and decreased range of motion.
Imaging Findings
The radiographic study (Fig. 1) showed a rounded appearance of both humeral heads, as a result of internal rotation, forming the lightbulb sign. A bone defect on the medial side of each humeral head consistent with fracture and fragmentation was also evident.
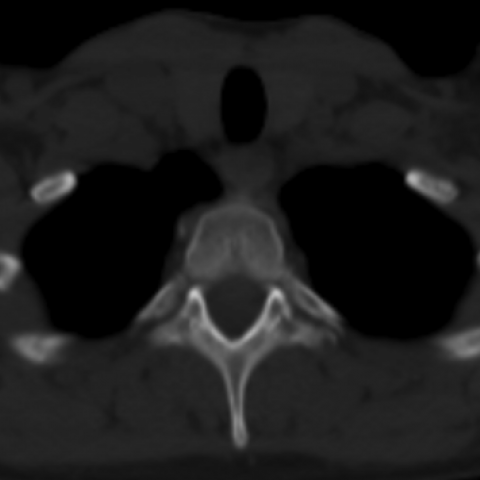
On CT (Fig. 2), apart from the posterior position of the humeral heads to glenoid, an impaction fracture of the anteromedial aspect of both humeral heads was obvious. Bone fractures, involving the lesser tubercles, and fragmentation were also confirmed. There were no bone glenoid lesions.
Imaging findings were compatible with a bilateral posterior shoulder fracture-dislocation, with reverse Hill-Sachs lesion. The patient was surgically treated with a bilateral McLaughlin procedure.
Discussion
Posterior shoulder dislocations account for only 2-4% of all shoulder dislocations and often occur as a consequence of a direct trauma, epileptic crisis or electrocution. In these two last conditions, bilateral dislocations are not infrequent, as a result of a more powerful contraction of internal rotator muscles during seizure, which leads to a more superior and posterior position of the humeral heads. Associated humeral head and glenoid lesions can occur due to continuous pressure between these structures [1-5].
Clinically, patients usually present with shoulder pain on a fixed internally rotated position. On physical examination there is a limited range of shoulder motion, mostly to external rotation and abduction [2].
Imaging findings on a frontal shoulder radiograph include loss of overlap between the humeral head and the glenoid, and an internally rotated humeral head, resulting in a rounded appearance that creates the lightbulb sign. Although findings on axillary view are usually obvious, this is rarely obtained because patients complain about pain to motion, as in our case [1].
While posterior shoulder dislocation can be difficult to diagnose clinically, as well as on radiographs, CT is often used to confirm the posterior position of the humeral head to the glenoid, as well as associated injuries such as fractures. Reverse Hill-Sachs lesion is an impaction fracture of the anteromedial humeral head, and it can be of surgical importance to identify and correct it, in order to prevent avascular necrosis. Usually, if the defect involves more than 25% of the humeral head, a surgical approach is preferred, as in the current case. Another complication, also present in this case, is a fracture involving the lesser tubercle which is anatomically related to the insertion site of the internal rotation of the shoulder [1,2,5].
Posterior shoulder dislocation is the most commonly missed major joint dislocation, frequently resulting in a delayed diagnosis that may result in shoulder instability, osteoarthritis and avascular necrosis [1,4,5]. Our case highlights the importance of a high level of suspicion for this diagnosis after a seizure. Follow-up of the case was lost after patient discharge.
Differential Diagnosis List
Final Diagnosis
Bilateral posterior shoulder dislocation with reverse Hill-Sachs lesion.
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Shoulder Radiographs

CT

Medical Imaging Analysis Report
I. Radiological Findings
1. On the anteroposterior (AP) view of the shoulder X-ray, the overlapping relationship between the bilateral humeral heads and the glenoid is abnormal. The humeral heads are displaced posteriorly and appear internally rotated, forming the so-called “lightbulb sign.”
2. The patient complains of pain and limited range of motion, making it difficult to obtain standard axillary or specialized views. However, based on the available images, the humeral head appears to be located posteriorly within the glenoid.
3. CT axial images show both humeral heads significantly positioned posteriorly, with a compressive fracture on the anteromedial aspect of the humeral head, suggesting a “reverse Hill-Sachs lesion.”
4. Additionally, there is evidence of a lesser tubercle fracture, potentially related to traction forces at the attachment site of the internal rotator tendons of the shoulder.
II. Potential Diagnoses
-
Bilateral Posterior Shoulder Dislocation:
The imaging findings (posterior displacement of both humeral heads, the “lightbulb sign,” etc.), along with the patient’s history of epilepsy and bilateral shoulder pain, suggest this diagnosis. Epileptic seizures can cause strong muscle contractions, and the dominance of the adductors and internal rotators predisposes to posterior dislocation. -
Accompanying Reverse Hill-Sachs Lesion:
A compression fracture of the anteromedial humeral head, commonly seen in posterior shoulder dislocations, related to impaction injury. Preoperative assessment is necessary to determine the extent of the lesion and decide on treatment. -
Accompanying Lesser Tubercle Fracture:
The lesser tubercle is the attachment site for the internal rotator muscles. During posterior dislocation, strong traction or impact by these muscles can lead to local avulsion or fracture.
III. Most Likely Final Diagnosis
Taking into account the patient’s history of epilepsy, recent seizure episode followed by bilateral shoulder pain and limited mobility, and the X-ray and CT findings, the most likely final diagnosis is “Bilateral Posterior Shoulder Dislocation Following a Seizure, Accompanied by Reverse Hill-Sachs Lesions and Lesser Tubercle Fractures.” Given that part of the humeral head defect could be significant (>25%), close evaluation is necessary to determine whether surgical intervention is indicated.
IV. Treatment Plan and Rehabilitation Program
1. Treatment Strategy:
(1) Closed Reduction: Mild to moderate posterior dislocations may be attempted via manual reduction under adequate anesthesia and muscle relaxation, followed by imaging confirmation.
(2) Surgical Treatment: If the reverse Hill-Sachs defect exceeds 25% of the humeral head volume, or if there is severe joint surface damage or significant fragment displacement of the lesser tubercle, surgical reduction should be considered. Bone grafting or arthroplasty may be employed to restore joint stability and reduce long-term complications.
(3) Postoperative Immobilization: After either closed reduction or surgery, shoulder braces or bandaging may be used, depending on the specific injury, to limit motion and ensure proper healing.
2. Rehabilitation/Exercise Prescription (FITT-VP Principle):
(1) Early Phase (1–2 weeks post-reduction or post-surgery):
• Main Goal: Reduce pain and prevent secondary injury.
• Frequency: 2–3 times per day of gentle activity.
• Intensity: Perform passive or assisted active range of motion within a pain-free or mildly uncomfortable range.
• Time: 3–5 minutes per session, gradually increasing based on tolerance.
• Type: Under professional guidance, perform pendulum exercises, range-of-motion exercises (e.g., finger ladder/wall-walking), avoiding excessive external rotation or abduction.
• Progression: Gradually increase the range of motion based on swelling, pain, and functional status.
(2) Intermediate Phase (2–6 weeks):
• Main Goal: Improve joint range of motion and begin muscle strengthening.
• Introduce elastic bands or lightweight resistance exercises to strengthen the rotator cuff and scapular stabilizing muscles.
• Gradually increase external rotation and abduction range, but proceed cautiously to avoid re-injury.
(3) Late Phase (after 6 weeks):
• Main Goal: Restore normal shoulder function and strength, prevent redislocation.
• Gradually incorporate resistance training and aerobic exercise (e.g., stationary cycling or walking), avoiding direct impact on the shoulder.
• Athletes or individuals with specific occupational needs should undergo specialized functional training under the guidance of a physician and rehabilitation therapist.
(4) Individualization and Safety:
• If the patient has concerns about bone quality or cardiopulmonary function, seek specialized advice to modify exercise intensity and type.
• Ongoing monitoring of shoulder pain, swelling, and functional recovery is essential. The plan should be adjusted case by case.
Disclaimer: This report is a reference medical analysis based on current data and does not replace in-person consultation or professional medical advice. The patient should undergo treatment and rehabilitation under the evaluation and guidance of an orthopedic or sports medicine specialist. This report does not assume any medical risk or legal liability.
Human Doctor Final Diagnosis
Bilateral posterior shoulder dislocation with reverse Hill-Sachs lesion.