


A 26-year-old male resident doctor presented with decreased sensation and pain in his thumb, index and middle finger of right hand since one month. His symptoms aggravated during sports involving continuous hand movements, such as badminton. On examination, there was hypoesthesia in the median nerve distribution.
Initially, X-ray is advised for the right wrist, and it showed no obvious abnormality (Fig. 1).
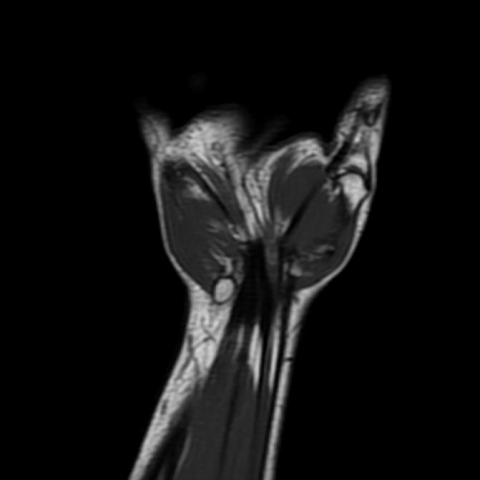
Also a magnetic resonance imaging (MRI) study of right hand with wrist was completed, and it revealed an intraneural lesion measuring approximately 10 x 5 mm with intralesional bleed in the median nerve in the carpal tunnel region. The lesion demonstrated iso to high signal intensity on T1W and hyperintensity on T2W and STIR sequences (Fig. 2, 3, and 4). On gradient echo image blooming was seen within the lesion suggestive of intralesional bleed (Fig. 5). On post-contrast examination, lesion showed significant heterogeneous enhancement (Fig. 6).
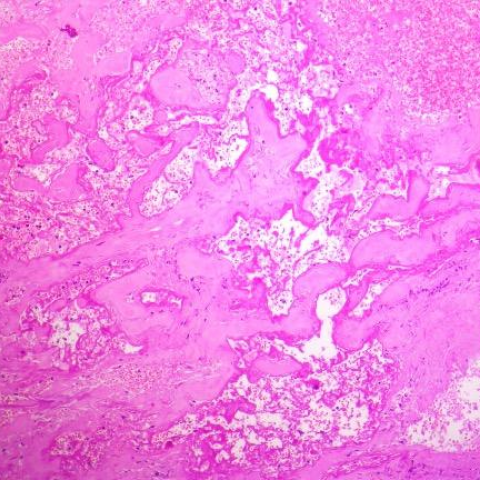
On histopathology the lesion was composed of intercommunicating ecstatic venous channels separated by thin fibrous stroma (Fig. 8). The lesion also showed medium to large cavernous spaces lined by a single layer of flattened endothelial cells with RBC's in lumen [2] (Fig. 9). Verhoeff-van Gieson stain for elastic fibres was negative (Fig. 10). Hence it was confirmed to be intraneural venous malformation of the median nerve [1].
Venous malformations of the median nerve are uncommon with only two cases being reported until now [1, 3]. These cases presented with features of Carpal Tunnel Syndrome [1].
Venous malformations comprise of masses of veins and venules lined by a single endothelial layer [2, 4] and they tend to form thrombosis often lead to forming phleboliths that are pathognomonic of venous malformations [5].
Ultrasound with color Doppler is the preferred diagnostic modality. MRI study is used to see the extent of lesion [5, 6]. However, plain MRI is not very sensitive in identifying small and deep venous malformations. Angiography can be useful in such cases [7].
The location and extent of the lesion determines the basis of treatment [1, 5]. Cryotherapy, sclerotherapy and laser therapy are used in treating the venous malformations but not effective in treating intraneural venous malformations [1]. Surgical corrections remain the treatment of choice [1].
In our case patient underwent surgery and on surgical exploration it revealed a bluish lesion with haemorrhagic foci involving the median nerve (Fig. 7). The lesion was removed completely by using microsurgical resection method, without damaging the nerve fibers [1]. No symptoms of median nerve compression were observed in the postoperative period.
Intraneural venous malformation of the median nerve [1].
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.














1. X-ray (Anteroposterior and Lateral Views of the Wrist): No obvious bone destruction or abnormal proliferation is observed. The articular surfaces appear normal with no definite signs of fracture or dislocation. The soft tissue contour shows no significant thickening or calcification.
2. MRI (Cross-sectional and Coronal Sequences of the Wrist/Forearm): A focal signal abnormality is seen in the right carpal tunnel and its proximal region. On T1-weighted imaging, this lesion appears intermediate or slightly low in signal; on T2-weighted imaging, it shows a relatively high signal, with some heterogeneous internal signal suggestive of vascular or thrombotic mixed signals. The lesion’s extent is consistent with the course of the median nerve, and there is a mild compressive effect on the nerve structure at that location. No obvious osseous infiltration is detected, and no extensive involvement of adjacent muscles is noted.
Considering the patient’s history, clinical presentation, and imaging features suggestive of a vascular lesion, all three diagnoses are possible. However, a vascular lesion merits particular attention.
Taking into account the patient’s age (26 years), chronic numbness and pain, worsening with movement, intraoperative findings, and pathological results indicating a “venous malformation,” the definitive diagnosis is a venous malformation (venous hemangioma-like lesion) within the median nerve.
This unique anatomical location and limited lesion involvement affecting the nerve fascicles explain the corresponding sensory and motor symptoms in the median nerve distribution.
After surgery and following symptom relief, the patient can gradually resume wrist and finger function exercises. It is advisable to follow the FITT-VP principle (Frequency, Intensity, Time, Type, Progression, and Individualization):
Throughout the rehabilitation process, close attention should be paid to pain, soreness, and any signs of local swelling. If significant swelling or recurrent nerve symptoms occur, seek medical advice and adjust the rehabilitation protocol accordingly.
This report provides a reference for medical analysis and is intended only for general information and advice. It does not replace in-person consultations or individualized guidance from qualified healthcare professionals. If you have any concerns or your symptoms worsen, please seek medical attention promptly for professional evaluation.
Intraneural venous malformation of the median nerve [1].