Giant cell tumour of tendon sheath: A rare case in the left elbow of a 8-year-old girl



Clinical History
An 8-year-old girl with good health complained of subacute onset of left elbow pain and denied any history of trauma.
Imaging Findings
Magnetic resonance imaging (MRI) of the left elbow revealed a relatively encapsulated localised 1cm x 2cm x 1.5cm nodular lesion in the olecranon fossa, showing intermediate T1 signal. T2 hypointense rim is noted, with relative heterogeneous content (Fig. 1, 2). No significant corresponding contrast enhancement is demonstrated. There is mild joint effusion with synovial thickening and enhancement. No associated cortical erosion or abnormal marrow signal is seen.
Discussion
Localised extra-articular giant cell tumour of tendon sheath (GCTTS) is classically seen to wrap around the tendons of the hand and fingers. The intraarticular form, also known as nodular synovitis, is similar to pigmented villonodular synovitis (PVNS) except in the degree of involvement of the affected joint, being more localised within the joint. Diffuse extra-articular GCTTS lesions are bigger and more aggressive and are found in an extra-articular location around large joints [1].
GCTTS usually affects people between 30 to 50 years and is more often seen in women. It is rare in children.
The extra-articular GCTTS usually presents with an increasing painless mass in the extremities, especially in digits on hand and foot. There is no specific symptom for GCTTS in the elbow [2, 3]. Therefore, the diagnosis of GCTTS would be difficult. Occasionally, the disease can lead to compression neuropathy and secondary osteoarthritis due to its mass effect.
In our case, the 8-year-old girl presented with elbow swelling and elevated inflammatory markers, which raises concern for underlying infective changes instead of neoplastic cause. Plain radiograph is usually not very helpful in the diagnosis of the disease.
Magnetic resonance imaging (MRI) is highly sensitive for identification and diagnosis of these lesions. It is usually seen as an oval, solitary mass with lobulated contours. It is intermediate or slightly hyperintense on T1-weighted images relative to skeletal muscle, whereas on T2-weighted images it shows variable signal intensity. It contains low signal intensity components due to haemosiderin deposits which are much more apparent on gradient echo images.
However, a definitive diagnosis can be made with pathological examination. It consists of fibrous tissue that contains pleomorphic cell population, including lipid-laden foam cells, multinucleated giant cells, and round or polygonal stromal cells, often with deposits of haemosiderin.
The standard of treatment for GCTTS is total excision of the tumour. When the tumour is localised, total excision is usually curative with a low rate of recurrence.
In conclusion, the occurrence of GCTTS of the elbow in a paediatric patient is an exceptional case as compared to those reported in previous literature. It is extremely difficult to make a proper diagnosis especially when it occurs in atypical sites or age groups. As the condition always presents with a lump, it should be considered as a differential diagnosis if the mass is found around joints. MRI would be useful for diagnosis when the symptoms of GCTTS are non-specific. Histopathological examination would remain the method for the definite diagnosis.
Differential Diagnosis List
Final Diagnosis
Localised form of giant cell tumour of tendon sheath
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
T2-weighted sagittal image of the left elbow

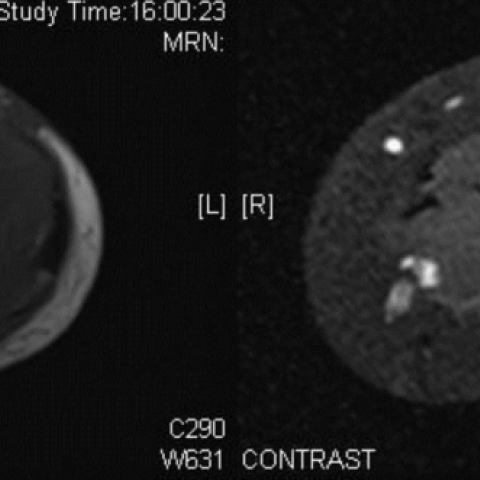
T1-weighted; post contrast T1-weighted axial images
Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided MRI images of the left elbow joint, there is a focal soft tissue mass observed around the joint, located near the extensor or flexor tendon sheath/synovium. On T1-weighted images, the lesion typically shows intermediate or slightly higher signal intensity. On T2-weighted images, the signal appears heterogeneous with low-signal components, potentially related to hemosiderin deposition. The lesion outline generally appears lobulated or as a relatively regular oval shape, with no evident erosive or destructive bony changes. Mild localized soft tissue swelling is noted, but there is no clear evidence of fracture or other severe soft tissue damage.
Certain sequences (such as gradient echo sequences) show localized low-signal deposits, suggesting the presence of hemosiderin. The mass margins appear relatively well-defined, with uniform or mild enhancement observed after contrast administration.
II. Potential Diagnoses
- Giant Cell Tumor of Tendon Sheath (GCTTS): This case is fairly consistent with the localized form of GCTTS, which commonly arises from tendon sheath and synovial tissue. On MRI, low-signal areas (due to hemosiderin) and mild to moderate enhancement after contrast are observed.
- Pigmented Villonodular Synovitis (PVNS): PVNS and GCTTS belong to the same pathological spectrum. PVNS is usually more diffuse involving the joint synovium, though localized lesions with similar low-signal deposits can appear. Differentiation lies in the extent of the lesion and overall joint involvement.
- Synovial Chondromatosis: Less likely to present with hemosiderin deposition, more commonly showing multiple cartilaginous nodules (which may show calcification or ossification on X-ray or CT).
- Infectious Synovium or Synovitis: Given that the patient once had elevated inflammatory markers, infection should be considered. However, imaging typically shows joint effusion or marked synovial enhancement, without the characteristic low-signal (hemosiderin) deposition seen here.
The above differential diagnoses are based on imaging characteristics and patient age. Among these, localized GCTTS is most consistent with a well-defined lesion surrounding the tendon or joint synovium with low-signal deposition.
III. Final Diagnosis
Integrating the patient's age, clinical features (localized swelling, mild pain, no significant history of trauma), imaging findings (mass signal characteristics and low-signal areas due to hemosiderin), and typical histopathological features (multinucleated giant cells, foam cells, and hemosiderin deposition), the most likely diagnosis is:
Localized Giant Cell Tumor of Tendon Sheath (GCTTS).
If further pathology confirms the diagnosis, it can be definitively established.
IV. Treatment Plan and Rehabilitation
Treatment Strategies:
- Surgical Treatment: Complete surgical excision is the primary strategy for localized GCTTS, typically resulting in a low recurrence rate. Surgical approaches can include open resection or arthroscopic-assisted resection, depending on the lesion size and location.
- Histopathological Examination: After surgical excision, a tissue sample should be sent for pathological examination to confirm the diagnosis and rule out malignancy.
- Other Treatments: If the condition is mild or the patient is not a surgical candidate, observation may be considered. However, for cases causing functional impairment or significant pain, surgery remains a reasonable option.
Rehabilitation/Exercise Prescription (FITT-VP Principle):
- Frequency: In the early postoperative period, after suture removal or wound healing, perform rehabilitation or physical therapy 3–4 times per week.
- Intensity: Begin with gentle flexion-extension movements and active range-of-motion exercises of the joint, avoiding excessive resistance or stretching. Pain should not be significantly exacerbated.
- Time: Each rehabilitation session can last 15–20 minutes initially and gradually increase to 30 minutes based on patient tolerance.
- Type: Include both active and passive range-of-motion exercises, flexion-extension practice, mild strength training (e.g., using resistance bands with small angles and low resistance), as well as soft tissue relaxation and self-massage around the joint.
- Progression: Once the wound is healed and joint range of motion has improved, resistance training and muscle strength/stability exercises can be gradually increased. The principle is to avoid pain or swelling exacerbation before escalating difficulty and intensity.
- Volume & Pattern: Each training session may consist of 3–4 sets of movements, with 10–12 repetitions per set and a 30–60 second rest between sets. If discomfort arises, reduce repetitions or intensity accordingly.
During rehabilitation, close attention should be paid to changes in pain, swelling, and range of motion. If significant discomfort or signs of recurrence appear, revisit your physician to assess for possible local tumor recurrence.
Disclaimer
This report is a reference analysis based on the currently provided information and does not substitute for in-person medical consultation or professional medical advice. If you have further questions or if your symptoms change, please seek medical attention promptly.
Human Doctor Final Diagnosis
Localised form of giant cell tumour of tendon sheath