Tumor of the chest wall in a young adult



Clinical History
An 18-year-old girl with a slow-growing mass in the right side of the chest, first noticed 1 year before.
Imaging Findings
A CT scan demonstrated a mass located between the fifth and sixth rib, originating from the 5th rib, with expansile growth and mineralisation.
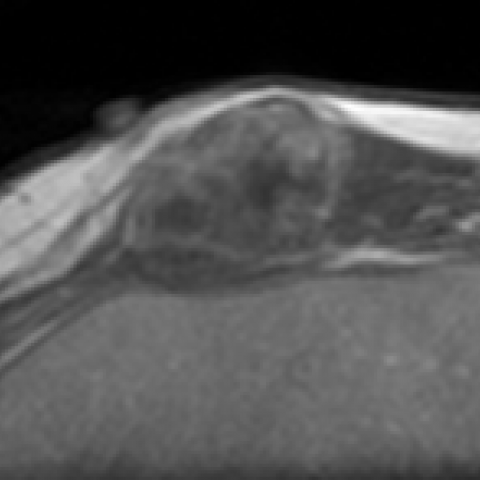
A MRI study showed a lobulated mass closely related to the costal chondroid tissue (5th and 6th rib).
The mass had an intermediate to low signal intensity on T1-weighted images and inhomogeneous predominantly high signal intensity on T2-weighted images. Dimensions were 24 x 36 x 31 mm (AP x LR x CC). Administration of intravenous contrast demonstrated peripheral enhancement.
Discussion
Chondromesenchymal hamartoma according to the latest WHO classification [4], also known as mesenchymal hamartoma of the chest wall or chest wall hamartoma [2], is an extremely rare, benign lesion with an uncertain pathogenesis. Chondromesenchymal hamartoma occurs mainly in early infancy and childhood [1]. It is usually solitary, but can be multifocal and even bilateral [2, 3, 5]. It arises most often on the right side and has a male-to-female ratio of 2:1 [3]. A chondromesenchymal hamartoma usually presents as a well-defined lesion arising within the medullary cavity or on the surface of a rib. Often contiguous ribs are affected [3].
Clinical manifestation depends on the size and specific location and ranges from a palpable or visible mass to severe respiratory distress due to compression of the lung [3].
On conventional chest studies, it appears as a mass arising from one or more adjoining ribs. The involved rib shows expansion, distortion and sometimes causes displacement of adjacent ribs. There is a variable degree of calcification [3]. In bigger lesions, secondary changes such as mediastinal displacement and scoliosis may be visible [3].
On CT it manifests as a bony lesion arising from the rib with osseous expansion and an associated extra-pleural soft-tissue mass with an inhomogeneous density and matrix mineralisation [7].
MRI usually shows heterogeneous signal on both T1- and T2-weighted sequences due to haemorrhage and cartilaginous components [7]. Haemorrhagic cystic regions with or without fluid-fluid levels due to secondary aneurysmal bone cyst formation are commonly visible [2].
This appearance on imaging is very similar to chondrosarcoma and often it is not possible to distinguish these two entities on imaging alone. The young age in combination with the location in the chest wall, however, favours the diagnosis of chondromesenchymal hamartoma.
A definitive diagnosis has to be verified by histopathological examination. Microscopically the lesions are composed of cartilage, fibroblastic regions and endochondral ossification. Focal stromal hypercellularity is often seen, but without atypia or abnormal mitotic activity [2]. Areas with blood-filled cystic spaces similar to aneurysmatic bone cysts are typically present [2, 4]. Different growth patterns are described in the literature varying from rapid growth, growth arrest to even reduction in size [6]. Surgical en-bloc resection is the treatment of first choice in symptomatic patients [2, 6].
Despite its sometimes alarming clinical, radiological and even histopathological appearance, chondromesenchymal hamartoma of the chest wall is a benign lesion, with an excellent prognosis after surgery.
Differential Diagnosis List
Final Diagnosis
Chondromesenchymal hamartoma of the chest wall
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
CT scan (sagittal reconstruction – soft tissue setting)

CT scan (soft tissue setting)

MR T1W sagittal

MR T2W axial

MR T2W axial fat-suppressed

MR T1W axial after intravenous contrast administration
MR T1W sagittal after intravenous contrast administration

Medical Imaging Analysis Report
I. Imaging Findings
The patient is an 18-year-old female presenting with a slowly growing palpable mass in the right chest, noted for approximately one year. Based on the provided CT and MRI images, the following findings are observed:
- The lesion is located in the right chest wall, originating from the rib, showing expansile change in the rib.
- CT reveals inhomogeneous density within the lesion, with local cartilage-like or calcified areas; it protrudes outward from the chest wall, forming a relatively well-defined mass.
- On MRI, the lesion demonstrates heterogeneous T1 and T2 signals; certain areas may show cystic or hemorrhagic signals, suggesting an aneurysmal bone cyst-like component.
- The lesion is fairly well demarcated from the surrounding soft tissue, with possible mild compression of the lung tissue, but no obvious signs of pulmonary invasion.
II. Differential Diagnoses
Based on the imaging features and patient history, the following diagnoses should be considered:
- Chondromesenchymal Hamartoma
Commonly occurs in children and adolescents, often involving the ribs and showing expansile growth. Imaging can reveal cartilaginous or mixed density/signal, frequently with hemorrhagic-cystic changes similar to an aneurysmal bone cyst, which aligns with most of the findings in this case. - Chondrosarcoma
Can also present with rib expansion and cartilaginous density/signal; however, it usually demonstrates more aggressive features and is more common in older patients. This lesion lacks obvious malignant signs and would require pathological examination for definitive differentiation. - Aneurysmal Bone Cyst (ABC)
Some imaging characteristics may overlap, but a pure aneurysmal bone cyst typically shows lytic bone destruction and often lacks a distinct cartilaginous matrix or calcification.
Considering the nature of the lesion (slow growth, cartilaginous component, patient’s age, etc.), chondromesenchymal hamartoma is the primary consideration, followed by chondrosarcoma or a lesion with an associated aneurysmal bone cyst component.
III. Final Diagnosis
Based on the patient's age (18 years), clinical presentation (a chronic, slowly enlarging chest wall mass), imaging characteristics (expansile rib lesion with mixed cartilaginous and cystic components), and relevant literature, the most likely diagnosis is:
Right Chest Wall Chondromesenchymal Hamartoma.
If there is any doubt or a need for confirmation, a pathological biopsy or intraoperative pathological evaluation should be performed for definitive diagnosis.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Surgical Treatment: For patients with symptoms or a progressively enlarging tumor, “en-bloc resection” is often the first-choice treatment. This procedure can effectively relieve pressure on the chest wall and lung tissue and prevent further lesion growth.
- Conservative Follow-up: If the lesion is small and asymptomatic, periodic imaging follow-up may be chosen after assessment by a specialist.
- Postoperative Follow-up: Regular imaging reviews are required after surgery to monitor for recurrence or residual disease.
2. Rehabilitation/Exercise Prescription Recommendations
According to the patient’s status post-surgery or during conservative management, a functional exercise plan should be progressively established based on the FITT-VP principles (Frequency, Intensity, Time, Type, Volume/Progression). An example is as follows:
- Early Postoperative Period (or Early Conservative Observation)
- Frequency: Light activities 1–2 times per day.
- Intensity: Maintain a low level without triggering pain or worsening fatigue, such as simple sitting or walking.
- Time: 5–10 minutes per session, gradually increasing.
- Type: Gentle breathing exercises, and flexion/extension of the lower limbs and the contralateral upper limb.
- Caution: Avoid excessive stretching or loading of the right chest.
- Mid-Level Postoperative Period (or Mid-Level Conservative Management)
- Frequency: 3–4 times per week.
- Intensity: Gradually increase to moderate intensity, with heart rate at about 50–60% of maximum.
- Time: 15–20 minutes per session.
- Type: Light strength training (e.g., small dumbbells or resistance bands) to enhance the shoulder girdle and core muscles, combined with gentle flexibility exercises.
- Caution: Closely monitor the surgical incision or lesion site for pain, and promptly inform the physician of any concerns.
- Late Postoperative Period (or Late-Stage Conservative Management)
- Frequency: 4–5 times per week.
- Intensity: Gradually increase to a moderate or moderately high level based on tolerance, but avoid high-impact exercises.
- Time: Around 30 minutes per session.
- Type: Focus on enhanced core stability and functional upper-limb exercises; incorporate low-to-moderate intensity aerobic exercises (e.g., stationary biking, brisk walking) and practice reasonable shoulder range-of-motion training.
- Caution: Discontinue exercise immediately and seek medical evaluation if chest wall pain, breathing difficulties, or any discomfort occurs.
The entire rehabilitation process should be conducted under the guidance of professional rehabilitation therapists or sports medicine specialists to ensure proper technique and avoid secondary injury.
Disclaimer
This report is based solely on the patient’s history and imaging information for reference purposes and does not replace an in-person clinical evaluation or expert opinion. Clinical diagnosis and treatment should be determined by a professional medical team following a comprehensive assessment.
Human Doctor Final Diagnosis
Chondromesenchymal hamartoma of the chest wall