A case of multiple thigh abscesses in a patient with multiple myeloma


Clinical History
A 59-year-old male patient with recently diagnosed multiple myeloma, confirmed on bone trephine, presented unwell with a chest wall mass. CXR and a subsequent CT chest abdomen and pelvis were performed. The patient then developed bilateral thigh pain and was unable to mobilise, MRI thighs was then also performed.
Imaging Findings
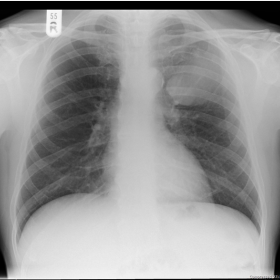
Figure 1. The chest X-ray shows a large left upper zone mass with an incomplete border sign indicating an extrapulmonary lesion.
Figure 2-3 CT chest revealed a 5x6 cm mass of soft tissue density arising from the anterior aspect of the left second rib. There were also several left axillary, supraclavicular and mediastinal pathological lymph nodes. Appearances of the soft tissue mass are suspicious of plasmocytoma in the context of known multiple myeloma. This was confirmed by histology obtained from ultrasound-guided core biopsy.
Figure 4-6 MRI both thighs: Multiple peripherally enhancing well-defined cyst-like lesions in the intramuscular plane, with no solid components identified. The largest lesion was in the right adductor magnus muscle belly measuring 9 cms. Differential diagnoses include multiple abscesses or neoplastic cystic metastases.
Discussion
Patients with multiple myeloma can mount a poor immune response to infection and therefore can present atypically. This patient had recently received pulsed dexamethasone as part of his multiple myeloma treatment, this may partly explain the atypical presentation of the multiple thigh abcesses.
At the time of the MRI, the patient did not have pyrexia or any other clinical sign of sepsis, the only clinical complaint was from pain from the local effects of the multiple abscesses. The lesions were not palpable or visible on inspection of the patient's legs. A dedicated MRI of the thighs was performed based on symptoms of pain and inability to mobilise, screening of other areas was not performed.
The distribution of the abscesses was unusual, there was no history of local trauma, injection or recent acute illness.
The MRI appearances of the multiple lesions were suspicious for abscess or malignant deposits; hence the need for ultrasound-guided aspiration in order to obtain a histological/microbiological diagnosis. Gram positive cocci (Staphylococcus aureus) were grown in the peripheral blood culture and the frank pus that was aspirated from one of the thigh lesions. An ultrasound-guided core biopsy of the chest wall lesion confirmed a diagnosis of plasmocytoma.
It is well documented in the literature that infection is a significant cause of mortality and morbidity in patients with multiple myeloma. [1-3] It has been observed that up to 45% of early deaths (within 6 months of diagnosis) were due to infection) [4]. It is thought that the underlying plasma cell disorder causes inherent immunodeficiency which leads to susceptibility to infection.
In this patient's case the early diagnosis of abscess was crucial, as this is a treatable condition if detected early enough. The patient presented atypically due to concurrent underlying imunosuppression (due to presence of multiple myeloma and recent dexamethasone treatment), in such patients atypical presentation of infection should always be considered.
Differential Diagnosis List
Final Diagnosis
Multiple thigh abscess and chest wall plasmocytoma
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Chest X-ray

CT: chest abdomen coronal

CT: axial chest soft tissue window

MRI: T1 axial + gadolinium

MRI: T2 fat saturated axial

MRI: T2 coronal

1. Imaging Findings
Based on the provided imaging (chest radiograph, chest-abdomen-pelvis CT, and thigh MRI), the main characteristics are as follows:
- Chest Imaging (X-ray and CT): A soft tissue mass shadow is visible in the chest wall, with an indistinct boundary. After enhancement, localized increased density is noted, showing slight demarcation from the surrounding tissue. Biopsy of this lesion later confirmed it to be an extramedullary plasmacytoma.
- Bilateral Thigh MRI: Multiple round-like abnormal signals are observed within the thigh muscles. They appear hyperintense on T2-weighted images, with varying degrees of surrounding edema. Some lesions suggest possible fluid pockets, and post-contrast scans show ring or septated enhancement, indicative of a fluid collection or abscess. These lesions do not exhibit typical bony destruction features, but involve muscle and soft tissue, with some areas showing significant localized edema.
In summary, the imaging appearance of the chest wall lesion strongly suggests a malignant tumor; the appearance of the bilateral thigh lesions is consistent with cystic or abscess-like changes.
2. Possible Diagnoses
Based on the medical history (diagnosed multiple myeloma and treatment with corticosteroids) and the imaging findings, the possible or differential diagnoses include:
- Multiple Myeloma with Extramedullary Plasmacytoma (Chest Wall)
The patient has already been diagnosed with multiple myeloma, and the biopsy-confirmed plasmacytoma in the chest wall is related to the course of multiple myeloma. - Bacterial Infection (Multiple Abscesses)
Patients with compromised immune function are susceptible to bacterial infections, particularly from gram-positive cocci such as Staphylococcus aureus, which can cause multiple soft tissue abscesses. The MRI findings (T2 hyperintensity, ring enhancement) are also consistent with abscesses. Microbiological tests (blood culture and aspirate) along with clinical pain presentation can further support this diagnosis. - Metastatic Tumor or Soft Tissue Sarcoma
Metastatic or primary soft tissue tumors can also present as soft tissue lesions on imaging. However, in this case, aspiration of pus and culture of Staphylococcus aureus indicated that an infectious process (abscess) is the most definitive diagnosis.
3. Final Diagnosis
Considering the clinical presentation, laboratory tests (positive blood culture, pus aspirate positive for culture), imaging features, and prior medical history, the following conclusions can be drawn:
- Confirmed multiple myeloma with a chest wall plasmacytoma
- Bilateral thigh multiple abscesses (main pathogen: Staphylococcus aureus)
As the patient’s immune system is suppressed due to multiple myeloma and recent corticosteroid use, any atypical infection must be taken seriously. Early detection and treatment of multiple abscesses are critical to improving prognosis.
4. Treatment Plan and Rehabilitation
4.1 Treatment Strategy
- Anti-infective Therapy: Select effective antibiotics based on the bacterial culture results (primarily covering Staphylococcus aureus), and adjust according to antibiotic sensitivity and clinical response.
- Abscess Management: For well-formed abscesses, consider ultrasound- or CT-guided aspiration and catheter drainage if there is a large volume of pus or continued formation. Smaller or more scattered lesions may be managed with close monitoring on anti-infective therapy, with interventional or surgical treatment if necessary.
- Underlying Myeloma Treatment: Follow standard treatment protocols for multiple myeloma (e.g., chemotherapy, corticosteroids, proteasome inhibitors, immunomodulatory drugs), maintain immune status, and monitor regularly.
- Supportive Care: Includes nutritional support, correction of anemia and electrolyte imbalances, as well as immunoglobulin replacement therapy if needed, to enhance infection resistance.
4.2 Rehabilitation and Exercise Prescription
Since this patient has multiple abscesses in the thigh region, rehabilitation exercises should be considered only after local inflammation and pain symptoms have improved. Overall, the recommendation is to follow a flexible, personalized, and gradual approach (FITT-VP principle).
- Early Rehabilitation (Post-Acute/Inflammation Control Phase):
- Frequency: 2-3 times a week, focusing on mild lower extremity activities.
- Intensity: Start with very low intensity (not exceeding daily living activity level) to avoid severe local pain or secondary injury.
- Time: 10-15 minutes per session, combined with simple range-of-motion exercises, such as leg lifts and knee extensions, gradually increasing.
- Type: Non-weight-bearing or reduced-weight-bearing activities are recommended, e.g., seated or supine joint movements, gentle isometric muscle contractions in bed or against a wall.
- Progression: Gradually increase exercise frequency and intensity based on pain control and resolution of inflammation.
- Mid-stage Rehabilitation:
- Frequency: Gradually increase to 3-5 times a week.
- Intensity: Maintain low to moderate intensity; begin simple resistance training (e.g., resistance bands, light weights) once abscesses and local inflammation are largely controlled.
- Type: May include static balance exercises (e.g., standing balance), shallow squats, or low-intensity cycling.
- Late-stage Rehabilitation (Functional Recovery Phase):
- Goal: Regain basic limb strength and joint flexibility, gradually returning to daily activities.
- Type: Moderate-intensity aerobic exercises (such as brisk walking, slow stair climbing), and appropriate strength training (like squats, band strengthening).
If significant pain or signs of local redness or swelling recur, prompt medical evaluation is advised, and intense weight-bearing or vigorous exercise should be paused.
Disclaimer: This report is a reference medical analysis based on the information provided and cannot replace an in-person consultation or professional physician’s individualized advice. For any questions or if symptoms worsen, please consult a specialist immediately.
Human Doctor Final Diagnosis
Multiple thigh abscess and chest wall plasmocytoma