Primary intraabdominal synovial sarcoma



Clinical History
A 56-year-old woman presenting to her general practitioner with a palpable, slowly growing and sometimes painful inguinal mass. The mass had been gradually increasing over the last year.
Imaging Findings
Initially the patient underwent an ultrasound exam that showed a heterogeneous mass deeper to subcutaneous cell tissue with AP axis larger than the transverse axis. It was predominantly hypoechoic and had internal vascularization. We performed a core needle biopsy showing a mesenquimal neoplasia suggesting synovial sarcoma.
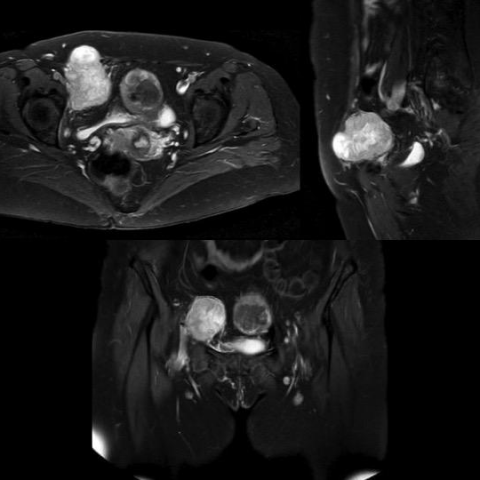
Subsequently, a thoracoabdominal CT was performed for initial staging that showed an intraabdominal but extraperitoneal lobulated well-defined heterogeneously enhancing mass with some hypodense areas probably necrotic or cystic component and solid pseudonodular enhancing component with some punctate hyperdensities that could be peripheral calcifications. A pelvic MRI and FDG PET-CT were performed for presurgical planning. The mass does not infiltrate adjacent anatomic structures, it is hypointense on T1 and shows the typical triple signal pattern on T2 and a solid nodular enhancing component, seen as well on the DWI and ADC maps. Another hypermetabolic lesion was seen in the right humerus, likely a metastasis.
Discussion
Synovial sarcoma is the fourth most common type of soft-tissue sarcoma, accounting for 2.5%–10.5% of all primary soft-tissue malignancies worldwide [1]. Synovial sarcoma originates from primitive mesenchymal cells and therefore is a malignant mesenchymal biphasic or monophasic neoplasm most often affects the extremities (80%–95% of cases) [1], particularly the lower limb around the knee. Despite its name, the lesion does not commonly arise in an intraarticular location but usually occurs near tendons ⁄ tendon sheaths and next to joint capsules. Synovial sarcoma also arises in areas with no obvious synovial or periarticular structures and has been described in almost all parts of the body thanks to the immunohistochemistry and demonstration of the t(X;18) chromosomal translocation or resulting SYT / SSX fusion gene transcripts, which is very specific for synovial sarcoma [1, 2]. It affects young adults with no gender predilection and manifests itself as a palpable and slowly growing mass that usually is > 5cm at the initial diagnosis. Primary intra-abdominal synovial sarcoma is rare, with less than 100 reported examples [3].
Histologic subtypes include three main variants: a classic biphasic type that has both a mesenchymal spindle cell component and epithelial component, a monophasic type (the most common) in which the spindle cells predominate and a poorly differentiated type [1]. Synovial sarcoma could present with calcifications, cystic changes and necrosis.
The imaging features of synovial sarcoma could be summarized as follows:
– CT: for initial staging. Non-infiltrative, well-defined mass often with punctate peripheral calcifications.
– MRI: for presurgical planning.
• T1: hypointense
• T2: triple signal pattern (hypo, iso, hyper to fat)
• Gadolinium enhanced: solid nodular enhancing component
– FDG PET-CT: to assess the efficacy of chemotherapy
The prognosis is poor because of the delay in diagnosis, which leads to local recurrence and metastasis. Only tumor size >5 cm is consistently associated with a poor outcome. Up to 50% of all synovial sarcomas recur locally, usually within 2 years, but sometimes many years later [2]. In fact, our patient had bone metastasis at the time of the diagnosis, confirmed with core needle biopsy.
The current treatment of choice is surgery, wide local excision (removal of the tumor, its pseudocapsule, and a normal cuff of surrounding tissue) without o with adjuvant therapy (if the margins are affected). The role of adjuvant therapy in the treatment of synovial sarcoma remains controversial. Chemotherapy has been used to treat metastatic or residual disease.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Primary intraabdominal synovial sarcoma with bone metastasis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Ultrasound and Doppler ultrasound study

Axial contrast-enhanced CT images

MRI study



PET-CT study

1. Radiological Findings
The patient is a 56-year-old male presenting with a palpable inguinal mass that has gradually increased in size and occasionally causes pain over the course of about one year. According to ultrasound and CT/MRI images, a relatively well-defined soft tissue lesion can be observed in the inguinal region, with heterogeneous density/signals internally. There is irregular or patchy enhancement in some areas, and Doppler ultrasound shows certain degrees of vascular flow within the lesion. On T1-weighted MRI, the lesion typically appears iso- or hypointense, while T2-weighted images reveal multiple signal intensities (the “triple sign”). Contrast-enhanced scans show irregular or septal-like enhancement. In some images, calcifications are noted. In addition, PET-CT indicates increased metabolic activity in the lesion, suggesting a high likelihood of malignancy.
2. Possible Diagnoses
Based on the patient’s age, the slow-growing nature of the soft tissue mass, and the observed enhancement pattern and metabolic features on imaging, the following differential diagnoses are considered:
- Synovial Sarcoma: Commonly seen around joints in the extremities, characterized by mixed signals on T2-weighted MRI and heterogeneous enhancement after contrast administration; calcifications may be present in some cases. Patients often experience slow growth, a palpable mass, and pain.
- Liposarcoma: May present clear fatty components on T1- and T2-weighted images; however, in the case of dedifferentiated or myxoid subtypes, the signal characteristics can be less typical.
- Undifferentiated Pleomorphic Sarcoma (UPS)/Malignant Fibrous Histiocytoma: Typically arises in the deep soft tissues of the extremities and trunk. Imaging often shows an irregular soft tissue mass with heterogeneous enhancement.
- Lymph Node Metastasis/Lymphoma: May manifest as an inguinal mass due to enlarged lymph nodes, but microscopic and PET-CT metabolic patterns may differ.
While these conditions can occur in the soft tissues or lymph nodes of the inguinal region, taking into account the imaging characteristics, minor calcifications, and the local anatomic features, synovial sarcoma is more likely.
3. Final Diagnosis
Based on the slow, progressive growth history, imaging findings (especially the “multiple signal intensities,” enhancement patterns on MRI, and high metabolic signal on PET-CT), combined with common histological and staining characteristics (including t(X;18) translocation or SYT/SSX fusion gene noted in the literature), the most likely diagnosis is primary synovial sarcoma in the inguinal region.
4. Treatment Plan and Rehabilitation
Treatment strategy:
- Surgical Treatment: The first choice is wide local excision (including the tumor with its pseudocapsule and a margin of normal tissue). If necessary, surrounding tissue and lymph nodes may be resected. If the surgical margin is involved, reoperation or adjuvant therapy can be considered.
- Radiation Therapy: Can be used as an adjuvant treatment, especially when margins are not clear or the lesion is large, helping reduce local recurrence.
- Chemotherapy: For patients with metastatic or residual disease, chemotherapy regimens containing anthracyclines can be considered to prolong survival and control metastasis, though results vary among individuals.
- Targeted and Other Therapies: Specific targeted therapies for synovial sarcoma are still under investigation; treatment decisions may depend on genetic testing results.
Rehabilitation/Exercise Prescription Recommendations:
- Early Postoperative Rehabilitation: Once the surgical site has healed and pain has subsided, begin with light active lower limb exercises and range-of-motion activities. The intensity should gradually increase based on patient tolerance.
- Transitional Phase: If surgery or radiation therapy has caused local soft tissue injury, start with mild lower limb strength training (e.g., leg raises, light resistance exercises) for about 10–15 minutes, 1–2 times per day. This can be supplemented by light aerobic exercises (e.g., using a stationary bike, gentle brisk walking) to maintain good cardiopulmonary function.
-
Long-Term Exercise and Functional Recovery (FITT-VP Principles):
• Frequency: 3–5 times per week
• Intensity: Begin at low to moderate intensity (where the patient may feel slightly out of breath but still able to converse), avoiding strenuous exercises.
• Time: Each session should be 20–30 minutes initially, with gradual increases based on individual capacity.
• Type: Low-impact aerobic activities such as swimming, using a recumbent bike, or walking on level ground, along with progressive resistance training.
• Progression: As tolerance improves, slight increases in exercise intensity or duration can be made every 2–4 weeks.
• Volume & Periodization: Adjust the total weekly training volume according to the patient’s recovery and lifestyle, ensuring adequate rest and nutrition. -
Important Notes:
- If significant swelling, worsening pain, or other discomfort occurs, discontinue training immediately and consult a healthcare professional.
- During chemotherapy or radiation therapy, coordinate treatment schedules with rehabilitation sessions to avoid excessive fatigue.
Disclaimer
This report is a reference medical analysis based on available information and does not replace an in-person consultation or physician’s professional diagnosis and treatment plan. Specific treatment decisions should be made and implemented by professional medical institutions according to the patient’s actual condition.
Human Doctor Final Diagnosis
Primary intraabdominal synovial sarcoma with bone metastasis