Pseudocyclops Lesion



Clinical History
A 24-year-old female presents with pain in her right knee for over a year. She had had previous arthroscopic reconstruction of the anterior cruciate ligament (ACL) of the same knee 5 years before in the context of a LCA rupture after a ski trauma.
Imaging Findings
The arthro-magnetic resonance imaging shows postsurgical changes with well-positioned bone tunnels and anterior cruciate ligament plasty.
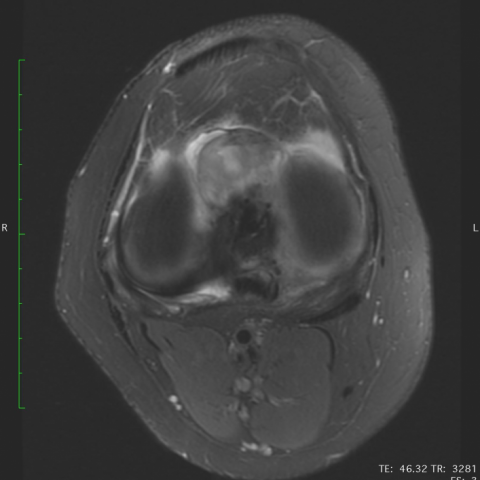
In the anterior intercondylar notch there’s a lesion resembling a cyclops lesion, with intermediate signal intensity on proton density and PD fat-saturated images (Figures 1-5). However, it doesn’t have the characteristics of arthofibrosis. Instead, it extends directly from the fixation tunnel, and it has a linear fibrillar morphology and signal characteristics that are compatible with an ACL. This is caused by a rupture of the ACL graft which subsequently folded anteriorly forming a folded stump which is called a pseudocyclops lesion.
Discussion
A. Background
After an arthroscopic reconstruction of the anterior cruciate ligament there are some possible complications. The complication rate is around 10-25% and include for example mechanical impingement, graft failure, arthrofibrosis, cystic degeneration of the graft, complications from the fixation materials and infection. [1; 2]
In the case of arthrofibrosis a granulation tissue is formed because of synovial hyperplasia and fibrotic tissue formation due to inflammatory changes [3].
Arthrofibrosis can be diffuse or localized. When the formed mass is located anteriorly to the reconstructed ACL it is called Cyclops lesion because of its arthroscopic appearance, and it’s a complication that happens in around 1-10% of the ACL reconstructions [3]
The Pseudocyclops lesion is a rare complication of the arthroscopic reconstruction of the ACL in which a partial graft tear occurs and subsequently the torn fibres are flipped anteriorly mimicking a Cyclops lesion. It is not an actual Cyclops lesion as it is a torn ACL instead of fibrotic tissue.
B. Clinical Perspective
The Pseudocyclops lesion, which is the torn graft located anteriorly in the intercondylar notch, can cause the same symptoms as a Cyclops lesion as it can cause a mechanical impingement, with loss of knee extension.
In these cases, an MRI exam is important to exclude other complications and to diagnose the graft tear with ACL folding and differentiate it from arthrofibrosis.
C. Imaging Perspective
MRI is the preferred imaging method for imaging the postoperative knee. [4]
Even with the postoperative changes, MRI is a useful noninvasive tool to examine patients with symptoms after ACL reconstruction, namely to detect Cyclops lesion which is a possible differen-tial diagnosis [5]. MRI also allows to detect other complications such as roof impingement, abnor-mal tunnel location, and graft tears [2].
The key finding of Pseudocyclops lesion is a linear fibrillary lesion with intermediate signal intensity located in the intercondylar notch resembling a torn ACL and in continuity with the remaining graft.
D. Outcome
The therapeutic option is arthroscopic repair of the graft tear.
E. Take Home Message, Teaching Points
- One of the complications of arthroscopic ACL repair is the formation of a fibrotic mass in the anterior joint recess, being this called “Cyclops lesion”.
- Another complication is graft tear with the torn fibres folding anteriorly and getting entrapped in the intercondylar notch, which is called a Pseudocyclops lesion as it resembles the fibrotic Cyclops mass.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Pseudocyclops Lesion
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Sagittal PD FSE FS image

Sagittal PD FSE image

Sag-Cor PD LCA image

Coronal PD FSE FS

Ax PD frFSE FS image
Medical Imaging Analysis Report
I. Imaging Findings
The patient is a 24-year-old female. MRI of the right knee shows the following main features after ACL (anterior cruciate ligament) reconstruction:
- In the femoral intercondylar notch where the reconstructed ligament is located, a local fibrous bundle-like structure is visible with heterogeneous signal, appearing as intermediate or slightly high signal on MRI. Some fibers appear torn and flipped anteriorly.
- No obvious, well-defined fibrous mass (commonly seen in the classic “Cyclops lesion” as scar or fibrotic tissue) is observed; instead, the torn fibers appear continuous with the residual ligament stump.
- No significant large-area cartilage defects observed at the patellofemoral or tibiofemoral articular surfaces. Joint effusion is not obviously increased.
- No noticeable abnormal masses or marked inflammatory changes in the surrounding soft tissues of the joint.
In summary, there is a partial tear of the reconstructed ACL with torn fibers flipped to the anterior aspect of the intercondylar notch, morphology similar to a traditional “Cyclops lesion” but essentially more consistent with a “Pseudocyclops lesion.”
II. Potential Diagnoses
- Pseudocyclops Lesion: Partial tear of the reconstructed ligament with some fibers flipped forward into the intercondylar notch, continuous with the residual ligament stump, consistent with MRI features in this case.
- True Cyclops Lesion: A mass of scar or fibrous tissue that usually does not show continuity with the ligament fibers. The main reason for excluding a “Cyclops lesion” here is that the torn fibers appear to connect with the residual ligament.
- Other Postoperative Complications: Such as simple postoperative ligament laxity, fixation material displacement, infection, or intra-articular loose bodies, none of which are clearly suggested on imaging.
III. Final Diagnosis
Considering the patient’s history of right knee ACL reconstruction, the current imaging findings, and clinical symptoms of persistent knee pain and difficulty in fully extending the knee, the most likely diagnosis is:
“Pseudocyclops lesion” (partially torn and flipped anterior cruciate ligament fibers, a pseudo-Cyclops lesion).
IV. Treatment Plan and Rehabilitation Program
1. Treatment Strategy
- Arthroscopic Exploration and Repair: If the tear is significant and associated with functional impairment, arthroscopic exploration and repair or revision reconstruction can be performed to restore joint stability and reduce mechanical impingement symptoms.
- Conservative Treatment: If symptoms are relatively mild and joint laxity is acceptable, bracing, physical therapy, and anti-inflammatory analgesic treatment may be considered. However, if the tear is large or symptoms are severe, conservative management is often less effective.
- Perioperative Rehabilitation: For patients requiring revision surgery, standardized rehabilitation before and after surgery is necessary to improve muscle strength and joint range of motion.
2. Rehabilitation and Exercise Prescription
Rehabilitation exercises should follow a gradual, individualized approach. The following is an example plan:
- Early Postoperative Phase (0-2 weeks):
- Main goals: Control swelling, reduce pain, and promote local blood circulation.
- Engage in passive or assisted range-of-motion exercises for the knee (limiting flexion-extension range to avoid overstrain).
- Mild isometric quadriceps contractions, ensuring no excessive load.
- Mid Postoperative Phase (2-6 weeks):
- Under professional guidance, gradually increase joint range of motion, aiming for near-normal flexion and extension.
- Strengthen the quadriceps and hamstrings with closed-chain exercises, such as partial squats and seated leg flexion-extension with low load.
- Maintain core stability and proprioception training, such as seated balance activities and balance board exercises.
- Late Postoperative Phase (6 weeks-3 months):
- Gradually increase strength training intensity and volume, including band-resisted squats, weighted straight leg raises, etc.
- Engage in low-impact aerobic exercises such as stationary cycling or elliptical training.
- If postoperative repair is stable, start light jogging or small-hop exercises at an appropriate time, ensuring joint stability and pain-free movement.
- Advanced Strengthening (3-6 months and beyond):
- After thorough assessment, progressively return to moderate or high-intensity sports.
- Continue strengthening the lower limb musculature and joint stability, for instance by increasing resistance with exercise bands, adding weighted squats, step training, and change-of-direction running drills.
- Ensure joint flexibility and muscle balance to prevent reinjury.
The entire rehabilitation process should monitor knee pain, swelling, and range of motion. Adjust training intensity and methods under the guidance of a physician or physical therapist as needed.
Disclaimer: The content of this report is for reference only and cannot replace an in-person consultation or professional medical advice. Patients should consult a specialist for further examination and treatment decisions based on their individual condition.
Human Doctor Final Diagnosis
Pseudocyclops Lesion