Bilateral empty and shallow bicipital groove



Clinical History
A 20-year-old woman, with no significant past medical history, presented with left shoulder pain that exacerbated with exercise over a three weeks period. There was no trauma or shoulder dislocation history. The physical examination showed no abnormalities and an MRI was requested for further investigation.
Imaging Findings
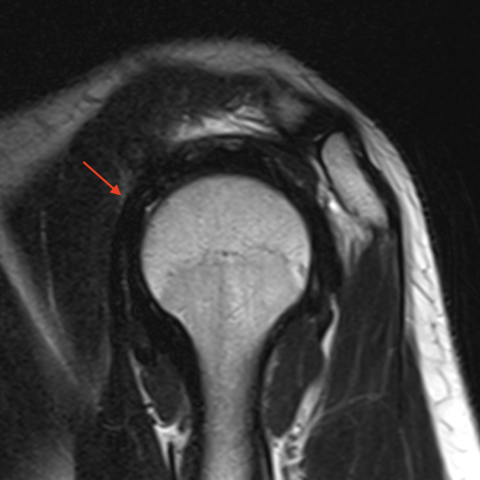
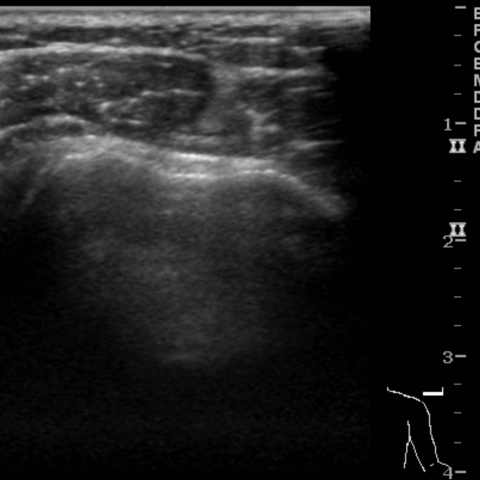
Left shoulder MRI showed an empty shallow bicipital groove with a normal robust short head of the biceps tendon (SHBT). There were no other significant findings and there were no signs that the absence of the long head of the biceps tendon (LHBT) was due to a tear, namely there was no intraarticular stump, no abnormalities on the usual topography of the biceps anchor and no fluid in the bicipital groove. Agenesis of the left LHBT was diagnosed and the patient was recalled for an ultrasound which confirmed similar findings on the right shoulder with an empty shallow bicipital groove establishing a diagnosis of bilateral agenesis of the LHBT.
Discussion
The biceps brachii has two muscle bellies with two corresponding proximal tendinous origins, the LHBT originates intraarticularly from the supraglenoid tubercle and posterosuperior labrum while the SHBT originates from the coracoid process. Distally the two bellies unite to form one tendon that inserts on the radial tuberosity [6,7]. The LHBT is known for having many anatomic variants, mostly derived from supernumerary heads, also termed accessory fascicles, that occur in 9.1-22.9% of the population, the most common of which is a supernumerary head that arises from the humeral shaft (10% of European whites). The LHBT can also present with additional origins from the articular capsule, humeral tuberosities and even the supraspinatus tendon, some of which can result in a bifid LHBT appearance promptly identifiable on MRI [5,7]. Although the incidence of LHBT congenital agenesis is unknown, it is believed to be extremely rare. Increasing use of MRI and arthroscopy has increased the incidence of this diagnosis. Kumar et al recently reviewed 35 cases, of which only 8 patients had bilateral agenesis [1,2]. Agenesis of the LHBT is a rare challenging diagnosis for a clinician since there are no specific symptoms, Popeye sign is absent and most clinical tests for evaluation of the LHBT, such as the speed test and the Yergason’s test, lack specificity for agenesis. The presentation of these patients is variable, they can be asymptomatic or may complain of shoulder pain or instability and imaging findings may be normal or show cuff or labral pathology. Although some report that shoulder pain may be related to LHBT agenesis alone, it is still uncertain, due to low levels of evidence available, whether the agenesis is just an incidental finding or if it may be the source of shoulder pain and even represent a risk factor for shoulder instability and labral tears [1,3,4]. On MRI an empty bicipital groove usually raises suspicion of LHBT tear. One should be aware of the rare finding of agenesis mainly when there is a shallow bicipital groove and no ancillary findings of LHBT tear, such as an intraarticular tendon stump, a fluid-filled tendon sheath and muscle oedema. Finally, it is important for us radiologists to be aware that a tear is not the only cause of an empty bicipital groove. Kumar et al reported that on 60% of cases, which were diagnosed during arthroscopy, agenesis of the LHBT was initially missed on MRI and later confirmed retrospectively [1]. Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Bilateral agenesis of the long head of the biceps tendon
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures



1. Imaging Findings
Based on the MRI of the patient’s left shoulder, the following main features are observed:
- In the intertubercular (bicipital) groove of the humerus, there is no typical signal of the long head of the biceps tendon; the groove appears relatively shallow and flat.
- There are no obvious signs of tendon rupture, such as high-signal fluid within the tendon sheath, proximal muscle edema, or retraction of the tendon stump.
- The rotator cuff muscles appear generally intact without evident tears or localized structural damage; no significant morphological abnormalities are noted in other bones or soft tissues around the shoulder joint.
2. Potential Diagnoses
Considering the patient is a young female with shoulder pain, no history of trauma or shoulder dislocation, MRI findings indicating an “empty cavity” in the bicipital groove, absence of fluid in the tendon sheath, and no clear signs of tendon rupture, the following possible diagnoses may be proposed:
- Congenital absence of the long head of the biceps tendon (agenesis): This is a rare congenital variation in which imaging shows an absence of tendon tissue within the bicipital groove, which is often relatively shallow and flat; individuals with this condition typically do not present with the characteristic ultrasound or MRI findings of a tear.
- Complete tear of the long head of the biceps tendon: If it is an old injury, the bicipital groove may appear “empty,” but it is often accompanied by indirect signs such as fluid accumulation around the torn tendon stump, proximal muscle atrophy, or localized edema, which are not adequately supported by the current imaging.
- Other surrounding soft tissue abnormalities: For example, bursa or shoulder joint capsule pathologies. However, there is no significant indication upon careful MRI evaluation.
Given the lack of an acute trauma history, the stable appearance of an absence, and a lack of typical signs of tendon rupture, congenital absence is more likely.
3. Final Diagnosis
Based on the comprehensive analysis of the patient’s history, clinical presentation, and MRI findings, the most likely diagnosis is:
Congenital absence of the long head of the biceps tendon (LHBT agenesis).
As this condition is rare and may not cause obvious symptoms during routine examinations or daily activities, it is clinically necessary to rule out other shoulder pathologies (e.g., rotator cuff disorders or labral injuries). If symptoms persist or worsen, further arthroscopic evaluation may be considered to confirm the diagnosis.
4. Treatment Plan and Rehabilitation Program
For suspected or confirmed congenital absence of the long head of the biceps tendon, without evidence of other injuries to shoulder structures, conservative and rehabilitative treatments are typically the mainstay:
- Conservative Treatment: Mainly includes non-steroidal anti-inflammatory drugs (NSAIDs) to alleviate inflammation and pain. When pain is significant, physical therapy methods (such as local heat therapy or ultrasound therapy) can be used concurrently.
- Shoulder and Scapular Stabilization Training:
- Start with low-load, isometric exercises to improve the strength and coordination of the rotator cuff muscles (especially the supraspinatus, infraspinatus, teres minor) and scapular stabilizers.
- Gradually increase load and training difficulty according to the FITT-VP principles (frequency, intensity, time, type, progression, and individualization).
- For example, perform resistance exercises for shoulder external rotation and internal rotation three times per week, 2–3 sets each session, 8–12 repetitions per set, gradually increasing resistance or repetitions.
- Arthroscopic Evaluation and Surgery: If symptoms persist or signs of instability occur, arthroscopy may be considered to further confirm any potential rotator cuff or labral pathology. Congenital absence itself typically does not require surgical intervention unless there are other complications.
- Progressive Rehabilitation Exercises:
- Initial Phase: Low-impact, controlled joint movements (e.g., light resistance training with barbells or resistance bands).
- Intermediate Phase: Strengthen the rotator cuff and core musculature to enhance shoulder stability, gradually introducing light targeted upper limb weight-bearing exercises.
- Advanced Phase: Based on the patient’s symptoms and functional recovery, incorporate simulated throwing or swinging exercises, ensuring a gradual return to sports or daily activities without significant pain.
Important Considerations: A professional evaluation should be performed before commencing any rehabilitation exercises to prevent secondary injury. If pain worsens or shoulder function deteriorates during exercise, seek medical attention promptly.
Disclaimer: This report is solely a reference analysis based on the provided information, and does not replace in-person consultation or professional medical diagnosis and treatment. Please consult a qualified healthcare provider for any questions or changes in condition.
Human Doctor Final Diagnosis
Bilateral agenesis of the long head of the biceps tendon