A rare case of benign fibrous histiocytoma of the iliac bone



Clinical History
A 22-year-old female patient presented with pain and swelling in the left iliac bone with associated difficulty in walking for the past 6 months. No history of trauma. No complaints of fever.
Imaging Findings
Radiograph of the pelvis shows an expansile lytic lesion with few bony septations and cortical disruption in the left iliac bone. There is no evidence of periosteal reaction and marginal sclerosis. (Fig. 1)
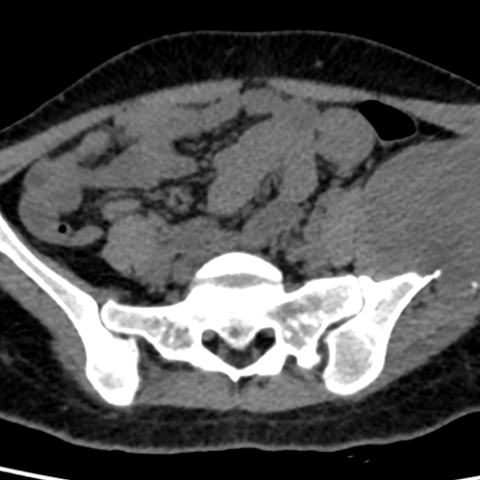
Computed tomography of the pelvis shows a large homogeneous soft tissue density (35-40HU) lesion with destruction of the left iliac bone. It also displaces the adjacent muscles. There is no evidence of calcification and haemorrhage. (Fig. 2)
MRI pelvis in all three sections demonstrates a well-defined T1 and T2 hypointense lesion in the left iliac bone with no diffusion restriction and blooming. Post-contrast images show peripheral enhancement of the lesion with a central non-enhancing area. There is no surrounding bony or muscle oedema. (Fig. 3).
Based on these findings, the diagnosis of fibrous tumour of the bone was made. The patient underwent left hemipelvectomy and biopsy revealed benign fibrous histiocytoma of the iliac bone.
Discussion
Benign fibrous histiocytoma (BFH) is a tumour with fibroblastic and histiocytic components accounting for less than 1% of all benign bone tumours [1]. This tumour is also known as fibroxanthoma or xanthogranuloma of the bone. Histologically it is composed of spindle-shaped fibroblasts, arranged in a storiform pattern, with a variable admixture of small, multinucleated osteoclast-like giant cells. Hence it is indistinguishable from non-ossifying fibroma. [2].
BFH occurs most commonly in young adults with female predominance. Most often it is asymptomatic, few individuals may present with pain. The most common locations include: The spine and the long bones, especially femur and tibia, preferably in a non-metaphyseal location. It is rarely identified in ribs, facial bones and pelvis [3].
On imaging, it displays cortical expansion with bony septations or ridges giving it a typical “soap bubble” appearance in radiographs. It is not associated with periosteal reaction or matrix calcification. Two third of cases show sclerotic margins. CT demonstrates its expansile nature, cortical disruption and associated soft tissue component. On MRI the lesion is hypointense on T2W images because of its fibrous nature. The closest differentials of BFH are non-ossifying fibroma and giant cell tumours (GCT), radiologically as well as histologically. However, we can differentiate them based on the following characteristics:
- NOF occurs in children, generally asymptomatic except in case of pathological fracture. It is metaphyseal in location and self-limiting. On the contrary, benign fibrous histiocytomas are frequently seen in young adults, come to notice because of pain and show non metaphyseal distribution.
- GCT is rare in children and adolescents less than 15 years of age, occurs after skeletal maturity, lacks sclerotic margins and shows soft tissue infiltration. On the other hand, BFH can have sclerotic margins and lacks soft tissue extension.
Other differentials on conventional radiographs are chondromyxoid fibroma (CMF) and aneurysmal bone cyst (ABC). T2W images differentiate CMF from BFH by showing high signal intensity in CMF due to its chondroid matrix. Aneurysmal bone cyst demonstrates typical multiloculated appearance and fluid- fluid levels on CT and MRI, which are absent in BFH [4, 5].
Complete surgical resection with curettage is the treatment of choice for BFH. Few cases might have an aggressive nature and show recurrence. It is of utmost importance to differentiate NOF from BFH as it requires no treatment.
Benign fibrous histiocytoma should be considered in differential diagnosis along with giant cell tumour, Aneurysmal bone cyst, Fibrous dysplasia and NOF in case of young patients presenting with expansile osteolytic lesion.
Differential Diagnosis List
Final Diagnosis
Benign fibrous histiocytoma of the left iliac bone.
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Radiograph of pelvis with both hips

Computed tomography of pelvis



MRI of pelvis






1. Imaging Findings
Based on the provided X-ray, CT, and MRI images, an expansile and destructive bone lesion is noted in the left iliac bone. The imaging characteristics include:
- On X-ray: The lesion appears round or irregular in shape with relatively well-defined margins. There are “soap-bubble” like multi-septations within the lesion, and thinning of the local cortical bone.
- On CT: The lesion presents as an expansile lucent area with mostly clear boundaries and possible sclerotic rims locally. No obvious intralesional calcifications or new periosteal reactions are observed.
- On MRI: The lesion shows intermediate to low signal intensity on T1-weighted images and relatively low or slightly high signal intensity on T2-weighted images (attributable to fibrous tissue). After contrast enhancement, mild to moderate enhancement is noted, without evidence of significant soft tissue infiltration.
No marked swelling or abnormal enhancement is identified in the adjacent soft tissue. The hip joint structure remains intact, with no clear joint surface destruction or widespread “punched-out” lesions. Overall, the lesion is predominately fibrous, well-demarcated, locally expansile, and associated with cortical thinning.
2. Possible Diagnoses
Considering the patient’s age (22 years old), symptoms (pain and swelling in the left iliac bone, without history of trauma or fever), and the imaging findings, possible differential diagnoses include:
- Benign Fibrous Histiocytoma (BFH): Also known as fibrous xanthoma. Commonly seen in young adults, it often appears as an expansile bone lesion with clear margins on imaging, sometimes showing a “soap-bubble” pattern. Fibrous components typically display lower signal on T2-weighted MRI.
- Non-ossifying Fibroma (NOF): Frequently found in children or adolescents, usually located at the metaphysis, often asymptomatic or incidentally discovered. It may resolve spontaneously. In adults with pronounced symptoms and atypical locations, the likelihood is lower.
- Giant Cell Tumor (GCT): Most common in individuals 20–40 years old, typically involving the epiphysis and extending to the subchondral bone. Imaging often shows less well-defined borders, a lack of a clear sclerotic margin, and possible soft tissue involvement.
- Aneurysmal Bone Cyst (ABC): Often demonstrates a “blow-out” or “bubble-like” expansile pattern. On CT or MRI, septations and fluid-fluid levels may be present. However, this case lacks the classic fluid-fluid levels.
- Chondromyxoid Fibroma (CMF): May show chondroid matrix signal features (high signal on T2). The relatively low T2 signal in this case does not fully match CMF characteristics.
3. Final Diagnosis
Combining the patient’s age, clinical presentation (gradual onset of pain and gait difficulty), imaging features (well-defined expansile lesion with predominantly lower T2 signal intensity), and the low-grade or benign nature thereof, the most likely diagnosis is:
Benign Fibrous Histiocytoma (BFH).
If there is any further doubt or to exclude other rare pathologies, a biopsy or surgical pathology examination may be indicated for definitive confirmation.
4. Treatment Plan and Rehabilitation Strategy
- Treatment Strategy
- If diagnosed as BFH with significant symptoms, surgical curettage of the lesion may be considered. Bone grafting may be performed if necessary.
- For smaller lesions without notable functional impairment or severe pain, conservative observation under close supervision by a specialist may be an option.
- In cases of aggressive lesions or repeated recurrences, more extensive surgical resection should be considered based on individual circumstances.
- Rehabilitation and Exercise Prescription
- Early Phase (within 1–2 weeks post-surgery or acute phase): Focus on reducing weight-bearing stress and protecting the affected iliac bone. Exercises should involve non-weight-bearing activities such as supine leg lifts and mild pelvic/core muscle training. Avoid strenuous movements or overloading.
- Intermediate Phase (functional recovery, ~2–6 weeks post-surgery): Gradually increase lower limb weight-bearing within a tolerable range of pain. This may include seated or standing resistance exercises, partial squats, or wall sits. Emphasize low resistance but higher repetition to strengthen muscles safely.
- Late Phase (strengthening, ~6–12 weeks post-surgery): Depending on bone healing status and specialist recommendations, incorporate moderate-intensity aerobic activities (e.g., walking, stationary cycling). Gradually increase resistance training, with special attention to key muscle groups such as the gluteal muscles and iliopsoas.
- Maintenance and Progression (12 weeks and beyond): Upon confirmation of stable bone healing, gradually increase the intensity and complexity of exercises (e.g., light jogging, core stabilization exercises, and progressive lower limb resistance training). Continuously monitor the tolerance of the affected iliac region.
FITT-VP Recommendations:
- Frequency (F): 3–5 sessions per week, adjusted to daily living patterns.
- Intensity (I): Start with low intensity, progressing to moderate; allow for some reserve in each session.
- Time (T): Each session approximately 30 minutes, gradually extending to 45–60 minutes based on tolerance.
- Type (T): Emphasize low-impact aerobic exercises (e.g., walking, swimming) combined with resistance training, focusing on bone and joint protection.
- Progression (P): Increase training intensity or duration once symptoms improve, pain is controlled, and imaging indicates good healing.
Disclaimer
This report is a reference analysis based on the provided clinical and imaging information and does not substitute for an in-person consultation or professional medical advice. Specific treatment and rehabilitation plans should be individualized and carried out under the guidance of relevant specialists.
Human Doctor Final Diagnosis
Benign fibrous histiocytoma of the left iliac bone.