Dermatofibrosarcoma protuberans with necrotic degeneration



Clinical History
A 57-year-old male patient with a history of a neglected subcutaneous mass located in the left mid-thigh for almost two years, presents for recent changes in the aspect of the overlying skin, which consisted of ulceration and active bleeding.
Imaging Findings
The MRI sequences show a well-defined ovoid mass measuring 33/41/55 mm (tr/ap/cc) located subcutaneously at the postero-lateral aspect of the left mid-thigh, associated with mild edematous infiltration of the surrounding subcutaneous tissue. The lesion demonstrates an intermediate signal on T1WI (compared to the muscle) and high signal on T2WI/STIR, with moderate heterogeneous enhancement on post-contrast studies, which suggests intratumoral necrosis. On post-contrast studies there is also visualisation of the cleavage plane with the underlying biceps femoris muscle and ilio-tibial tract.
Discussion
Dermatofibrosarcoma protuberans (DFSP) is a rare dermal tumour with an incidence rate of 0.8 to 4.5 cases per million persons per year, occurring most frequently in 30-40-year-old adults, without a gender-related predominance. It manifests a low metastatic rate but, a significant subclinical locally aggressive behaviour. [1,6]
Clinically, DFSP typically presents as an asymptomatic, slow-growing red-brown indurated plaque which eventually develops multiple nodules. Rarely it can ulcerate and bleed, as in the present case. DFSP is known to have implacable growth with profound projections which cannot be assessed on clinical exam, hence the importance of the imaging examination. [2,3]
On imaging studies, DFSP commonly appears as a well-defined nodular mass involving the skin and subcutaneous tissue. Ultrasound is essential for the primary evaluation of such superficial masses: characterizes its size, structure (solid vs cystic), vascularity, compressibility, extent. It is used as the initial imaging modality because of its availability, portability, and low cost. [5]
In our case, the lesion appeared as a heterogeneously hypoechoic solid mass, with significant posterior acoustic enhancement, which made it impossible to appreciate its deep limits. Therefore, MRI was the next step.
On CT, it shows soft-tissue attenuation values. On MRI it appears hyperintense on T2-WI and PD and hypointense on T1-WI, with suppression on fat-saturated sequences. Both on CT and MRI the lesion may exhibit heterogeneous contrast enhancement, as it undergoes necrotic or cystic degeneration. [2,4]
An important feature for the therapeutic attitude is the tumour's infiltration into the adjacent structures. In our case, MRI indicated a cleavage plane towards the muscular compartment, which is a favourable feature for a clean excision with little chance of recurrence, hence the justified decision for surgical removal of the mass, with post-op histopathological examination.
Imaging studies are not specific, since they may not distinguish DFSPs from other soft tissue sarcomas. Therefore, histological examination is the only definitive diagnostic method. [4]
The immunohistochemical examination is also decisive in the differential diagnosis of other tumours. [3]
The treatment is surgical, taking into consideration the high rate of local recurrence.
DFSP typically originates in the dermis and tends to infiltrate the underlying structures. In our case, the tumour was confined to the skin and subcutaneous tissue, but presented with ulceration and necrotic degeneration. When facing a superficial tumour with such clinical and imaging properties, it is important to take into consideration the diagnostic of DFSP, even in the presence of rare complications.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
The lesion was histo-pathologically proven to be a dermatofibrosarcoma protuberans
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
T2 STIR coronal

T1 coronal

T1 FS pre-contrast (3a) and post-contrast (3b)


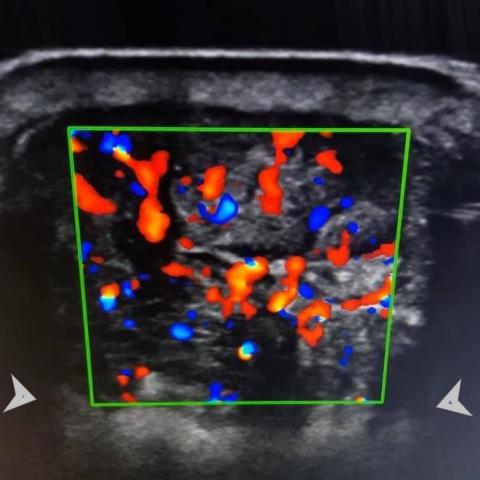
Colour Doppler ultrasound
Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided ultrasound and MRI results, the lesion is located in the subcutaneous tissue of the mid-left thigh. It appears solid and irregular in shape with the following characteristics:
- Ultrasound: Shows a heterogeneous hypoechoic mass with abundant internal blood flow signals and posterior acoustic enhancement. The actual depth range of the lesion is difficult to accurately determine by ultrasound.
- MRI:
- On the T1-weighted images (T1-WI), the signal is relatively low, with regions of heterogeneous signal at the margins, suggesting possible necrosis or cystic changes inside.
- On the T2-weighted (T2-WI) and PD images, the lesion shows markedly high signal intensity, with focal high-signal areas indicating complex internal components.
- The lesion is mainly located in the subcutaneous layer, with an apparent compressive or potentially infiltrative effect toward the deeper soft tissues. However, MRI shows a relatively clear boundary with the muscle layer, and no obvious muscle invasion is observed.
- After contrast enhancement, the lesion shows heterogeneous enhancement, consistent with common characteristics of soft tissue tumors.
The overall assessment indicates locally infiltrative growth with a close relationship to surrounding tissues, and the skin surface shows ulceration and bleeding changes.
II. Differential Diagnosis
Taking into account the patient’s history (a 57-year-old male with a long-standing subcutaneous mass in the left thigh, recently exhibiting skin ulceration and bleeding) and the imaging presentation, the following should be considered:
- Dermatofibrosarcoma Protuberans (DFSP): This tumor commonly arises in the skin and subcutaneous tissues, grows slowly but has locally invasive potential. On MRI, it often appears as a solid mass with low T1 signal and high T2 signal, and may exhibit necrosis, cystic changes, and heterogeneous enhancement. Clinically, tumor enlargement, bleeding, or ulcer formation may occur.
- Other Soft Tissue Sarcomas: For example, malignant fibrous histiocytoma or liposarcoma. These can also present as solid soft tissue masses with surface ulceration. Histopathological analysis and immunohistochemistry are needed for definitive differentiation.
- Deep Hemangioma or Angiosarcoma: An abundant vascular supply may be seen on ultrasound and MRI, but the imaging morphology and enhancement patterns often differ slightly. Pathological examination is required for clarification.
III. Final Diagnosis
Considering the patient’s age, the longstanding presence of the mass, recent skin ulceration and bleeding, and the subcutaneous infiltrative growth pattern on imaging along with MRI signal characteristics, the most likely diagnosis is Dermatofibrosarcoma Protuberans (DFSP). Since definitive diagnosis requires pathological and immunohistochemical confirmation, further postoperative histological and immunohistochemical examinations are essential to establish the diagnosis.
IV. Treatment Plan and Rehabilitation
1. Treatment Plan
- Surgical Resection: The primary treatment for DFSP is surgery, requiring adequate and complete tumor excision. If MRI suggests a distinguishable safe margin between the tumor and the muscle layer, every effort should be made to preserve muscle function, but adequate surgical margins must be ensured.
- Other Treatments: For cases with unclear margins or postoperative recurrence, adjuvant radiotherapy or molecular targeted therapy (e.g., tyrosine kinase inhibitors) may be considered, depending on pathological staging and individual circumstances.
2. Rehabilitation and Exercise Prescription
Following surgical resection and completion of treatment, the rehabilitation program should follow these general principles:
- Early Stage (1–2 weeks post-operation):
- Focus on protective training, ensuring basic maintenance of limb mobility and muscle strength.
- Gentle active or passive joint movements can be performed, avoiding excessive traction on the surgical area. Pain should remain within a tolerable range.
- Middle Stage (2–6 weeks post-operation):
- When the wound has healed well, begin low-intensity weight-bearing exercises, such as straight leg raises and isometric quadriceps strengthening.
- Gradually increase the range and duration of activities, 2–3 times daily, 15–20 minutes each session, while closely monitoring for swelling or pain.
- Late Stage (6 weeks post-operation and beyond):
- Progressively return to regular muscle strengthening and functional exercises according to individual needs, including walking and light strength training.
- Following the FITT-VP principle, gradually increase exercise frequency (3–5 times per week), intensity (from mild to moderate), and duration (gradually up to 30 minutes or more), with low-impact options like swimming or using a stationary bike. Monitor the surgical area closely.
- If there is limited weight-bearing capacity in the lower limb, targeted training under the guidance of a rehabilitation therapist or specialist is recommended to ensure safety.
Throughout the rehabilitation process, consider the patient’s overall condition, including any comorbidities (e.g., compromised cardiopulmonary function or low bone density), adjusting exercise intensity and scope accordingly to ensure a safe, individualized program.
V. Disclaimer
This report is based on the current imaging and clinical information provided, offering a reference analysis only. It does not replace in-person consultation or the treatment advice of a qualified medical professional. Patients should follow their specialty physician’s guidance, considering personal medical history, surgical results, and pathological findings, to determine the appropriate course of treatment.
Human Doctor Final Diagnosis
The lesion was histo-pathologically proven to be a dermatofibrosarcoma protuberans