Benign chondroid syringoma of the thigh



Clinical History
A 52-year-old woman with no relevant medical history was referred to the orthopaedic oncology clinic for assessment of a slowly growing, non-painful, non-tender lump in the subcutaneous tissue of the posteromedial thigh. This had been present for 4 years, measuring approximately 2cm in maximal diameter on clinical examination.
Imaging Findings
Ultrasound demonstrated a well-delineated heterogeneously hypoechoic lesion within the subcutaneous fat of the posterior thigh containing a small number of vessels on colour doppler (fig. 1a, 1b).
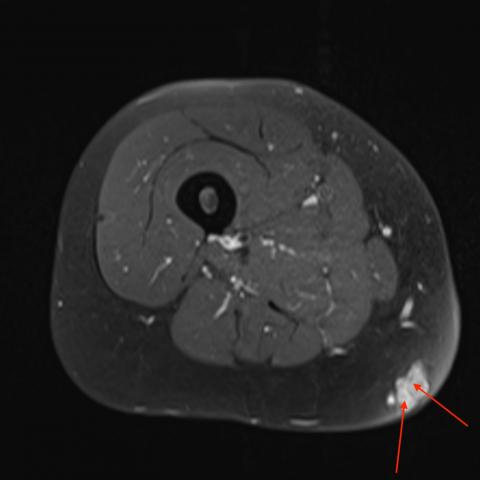
MRI including contrast sequences demonstrated a subcutaneous lesion extending to the skin measuring 2.1cm x 1.9cm x 1.3cm. This was largely intermediate signal on T1WI, with an incomplete peripheral low signal margin (fig. 2). Heterogenous high signal was observed on T2WI (fig. 3) and T1 TIRM sequences (fig. 4). Post-contrast, there was avid enhancement with some discrete internal, relatively hypoenhancing septations (fig. 5a, 5b). No calcifications were evident on MRI.
The lesion had no invasive features with no deeper underlying abnormality. Following percutaneous biopsy and subsequent marginal excision by the sarcoma surgeons, histology demonstrated a collagenous and myxoid background containing ductal structures and epithelial strands with some squamous differentiation, keratocyst formation, and focal calcification consistent with benign chondroid syringoma (CS).
Discussion
CS is a rare tumour of sweat gland origin (<0.01% of all primary skin tumours) usually occurring in the head and neck but also reported in locations including extremities, scrotum, eyelids and brain [1,2,3,4].
Presentation may be with a slowly enlarging lump with symptoms dependent on location [2,5]. Most cases are benign but rare malignant cases can occur which are typically invasive with a high rate of recurrence. Features concerning malignancy include extremity and torso origin, size >3cm and female gender [1,4,6].
Few reports focus on the imaging features of CS and most are MRI based. Benign lesions have been described as heterogeneous, isointense to muscle & low signal on T1WI, and heterogeneous and high signal on T2WI [3,5,6,7,8]. Kakitsubata et al described a lesion with a solid component containing chondroid material and fat, surrounded by fluid and an incomplete peripheral rim of low signal on T1, T2 and fat-saturated T2 sequences [7]. Kerimoglu et al described a lesion with focal high signal on T1WI, homogenous high signal on STIR and cystic components [6]. Fibrovascular septae have also been described [5]. In two cases post-contrast findings were not described [3,7]. Otherwise, enhancement is a consistent finding [5,6,8].
Ryu et al describe benign CS on ultrasound as a well capsulated hyperechoic mass with a central hypoechoic scar-like portion from which radiated hypoechoic hypervascular septa-like structures[5].
We found 2 cases describing malignant CS on imaging. Park et al reported a lesion of low signal on T1WI “higher than that of surrounding muscles” and heterogeneous signal on T2WI. However, review of their images demonstrates a heterogenous lesion on T1WI. They also describe peripheral low signal and heterogenous enhancement [2]. Nicolau et al reported heterogeneous predominantly intermediate signal on PDWI, heterogeneous internal high signal with peripheral intermediate signal on T2WI and heterogeneous high signal on STIR [9].
With limited reports, imaging characteristics of CS are nonspecific and there is overlap in the appearances of benign and malignant cases. Features such as heterogeneous signal on T1 & T2WI, enhancement and a peripheral rim of low signal are described in both. Imaging is however useful in narrowing the differential diagnosis and in our case diffuse enhancement, lack of macroscopic calcifications and no exophytic components made epidermoid inclusion cyst, pilomatrixoma and dermatofibrosarcoma protuberans less likely respectively. However, other malignancies including pleomorphic dermal sarcoma could look similar, ultimately necessitating biopsy for confirmation of diagnosis.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Benign Chondroid Syringoma
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures






Medical Imaging Analysis Report
1. Imaging Findings
Based on the ultrasound and MRI images, the lesion is located in the subcutaneous tissue layer of the medial posterior side of the left thigh, with a size of approximately 2 cm. Ultrasound shows uneven internal echoes of the lesion with relatively clear boundaries and partial blood flow signals. On the transverse T1-weighted MRI, the lesion is slightly low or isointense, while on the T2-weighted MRI, the signal is heterogeneously high with a low-signal rim in some areas. Contrast-enhanced scans reveal moderate to marked enhancement in the solid portion of the lesion, with no obvious infiltrative changes in the surrounding area.
- Lesion shape: Sub-round or oval, with relatively clear boundaries.
- Signal characteristics: Slightly low or isointense on T1, high signal on T2, showing heterogeneous enhancement inside.
- Size and location: Located in the thigh subcutaneously, moderate depth, about 2 cm, with no evident invasion into muscle or bone.
- Ultrasound blood supply: Color Doppler shows partial blood flow signals, indicating some blood supply to the lesion.
2. Possible Diagnoses
Given the patient’s age of 52, a subcutaneous lesion in the lower limb, and a four-year history of slow growth, along with imaging features, the differential diagnoses may include:
- Chondroid Syringoma
This is a rare sweat gland–derived tumor often presenting as a slowly growing subcutaneous nodule. MRI may show heterogeneous T1/T2 signals with enhancement. If located in the extremities, malignancy must be considered; however, in this case, the lesion is relatively small (approximately 2 cm) and has shown slow growth, suggesting a benign lesion. - Epidermoid Cyst
Commonly appears subcutaneously as a near-round cystic lesion. On T2-weighted images, it often appears with high signal intensity. If the cyst wall is calcified or contains keratin, characteristic signals may be seen. However, the enhancement and blood flow observed in this lesion do not fully align with an epidermoid cyst. - Pilomatrixoma
Can form nodules in the subcutaneous tissue, often with varying degrees of calcification or ossification density. On MRI, low-signal calcification areas may be seen. In this case, there is no obvious calcification visible. - Dermatofibrosarcoma Protuberans or Other Soft Tissue Sarcomas
May present with enhancement and heterogeneous T2 signal. They typically exhibit progressive enlargement in the subcutaneous or dermal layers, and some patients may have pain or skin adhesion. While this case shows heterogeneous signals, the slow growth and relatively well-defined boundary suggest otherwise.
3. Final Diagnosis
Based on the patient’s medical history, clinical presentation, and imaging characteristics, the most likely diagnosis is: Benign Chondroid Syringoma.
Because imaging features alone provide limited differentiation between benign and malignant forms, further tissue biopsy or surgical excision followed by pathological examination is recommended when feasible, to confirm the lesion’s nature.
4. Treatment Plan and Rehabilitation
1. Treatment Strategies
- Surgical Excision: For suspected or confirmed chondroid syringoma, most experts recommend complete resection to prevent recurrence. If intraoperative or postoperative pathology indicates malignancy, an appropriately wider excision should be considered.
- Follow-up Monitoring: If the lesion is initially presumed benign, regular imaging follow-up may be conducted to monitor changes in size and boundaries. However, considering the nature of the tumor, surgical removal is often the first choice.
2. Rehabilitation/Exercise Prescription
If the patient undergoes surgical removal or other local procedures, the rehabilitation and exercise prescription should be individualized based on assessments by the physician and rehabilitation therapist. In general:
-
Early Postoperative Phase (1–2 weeks):
- The main goal is to protect the surgical area and promote soft tissue healing.
- Low-load active joint movements of the lower limb can be performed under medical guidance, avoiding excessive tension at the incision site.
- Gentle in-bed exercises and short-distance walking are encouraged.
-
Mid Postoperative Phase (2–6 weeks):
- Focus on improving local muscle strength and joint flexibility, such as light resistance band exercises with small-range joint movements.
- Depending on wound healing status, gradually increase lower extremity weight-bearing training under the supervision of a rehabilitation therapist.
- Exercise frequency can be arranged 3–4 times per week, 20–30 minutes each session, at an intensity that does not cause significant pain or fatigue.
-
Late Postoperative Phase (6 weeks or more):
- Once local stability is ensured and there is minimal risk of recurrence, continue muscle strength, balance, and proprioception training.
- Gradually extend training time to 30–45 minutes per session, 3–5 times per week. Examples Include mild strength exercises, lower limb flexibility training, or stationary cycling.
- If the patient’s physical condition allows, transition to moderate-intensity exercises under guidance and consider additional physical therapy as needed.
The above plan follows the FITT-VP (Frequency, Intensity, Time, Type, Progression, and individualization) principles. Specific adjustments should be made based on the patient’s tolerance, the status of incision healing, and follow-up results.
Disclaimer: This report is a reference analysis based on imaging and clinical information. It should not replace an in-person consultation or the professional opinion of a qualified physician. Any specific treatment or rehabilitation plan should be carried out under professional medical guidance.
Human Doctor Final Diagnosis
Benign Chondroid Syringoma