Benign notochordal cell tumor of the sacrum



Clinical History
A 48-year-old woman with back pain was referred for an MRI (Magnetic Resonance Imaging) of the spine. She had no clinical records of oncological or hematological disease.
Imaging Findings
MRI of the lumbar spine showed a rounded focal lesion in the sacrum, 20 mm in diameter, centred in S1, without perilesional oedema. Its signal intensity was heterogeneous, intermediate/low on T1WI (T1 Weighted Imaging) and high on T2WI sequences. L5-S1 degenerative changes were also noted, with disc bulging. No other bone lesions were identified in the lumbar spine.
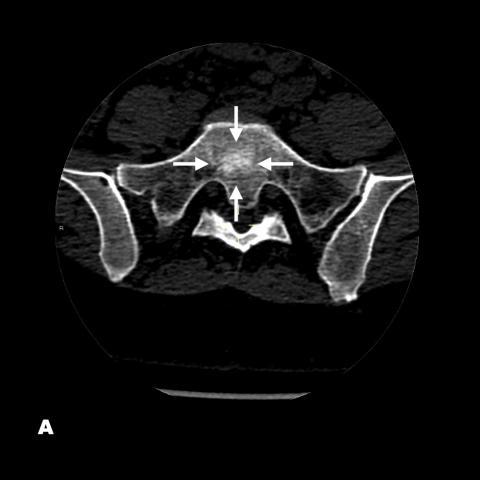
Given the finding of a bone lesion, the patient had a complementary Computed Tomography (CT) done, on which the lesion showed subtle sclerosis of imprecise margins, without signs of radiological aggressiveness.
On a follow-up MRI of the sacrum performed 3 months after the first MRI scan, the lesion remained stable and showed no post-contrast enhancement or soft tissue component.
Discussion
Benign Notochordal Cell Tumors (BNCT) are lesions of notochord cell origin. Histologically, they are differentiated from chordomas and notochord remnants and have recently been recognised as separate entities. They are frequent lesions on autopsies reported in about 20% of cadaveric specimens in the clivus and spine and are increasingly described in imaging studies.
Although most are asymptomatic and an incidental finding, cases associated with back pain have been reported.
On MRI, they are frequently found as rounded intraosseous lesions, characteristically well-defined and with low signal on T1WI and predominantly high signal on T2WI, although some hyperintense foci of intralesional fat may be found on T1WI. They do not show soft tissue mass or postcontrast enhancement. On X-rays, they are often unnoticed and even imperceptible, and on CT, when visible, they frequently show subtle hyperdensity, without osteolysis. They show little or no activity on bone scintigrams.
Although BNCT are considered benign lesions that do not require surgical resection, sporadic cases associated with chordoma have been described, and it is controversial whether they are concomitant lesions, or whether TBCN may occasionally act as a precursor to malignant chordoma-like lesions. Therefore, even when sacral lesions show typical features of BNCT, imaging follow-up is recommended to confirm their radiological stability.
In conclusion, BNCT are lesions increasingly described in imaging studies, usually as incidental findings. Knowledge of their characteristic imaging features is crucial for radiologists in order to differentiate them from malignant bone lesions that require more aggressive treatments. Searching for extraosseous extension, enhancement or soft tissue components are key findings to indicate biopsies and to rule out chordomas or other malignant tumours.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Sacral benign notochordal cell tumour
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures







Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided lumbar-sacral MRI and CT images, the following observations are noted:
- A well-demarcated lesion within the sacral vertebrae (at S1–S2 level);
- On MRI T1-weighted images (T1WI), the overall signal is low to isointense, with some small high-signal areas (possibly indicating fatty components);
- On MRI T2-weighted images (T2WI), the lesion shows relatively high signal intensity without obvious soft tissue masses or bone destruction;
- On CT scans, the lesion appears as a mildly high-density area, without significant bony destruction or cortical expansion;
- The lesion has a fairly clear boundary, and no obvious destruction of the vertebral structure or space-occupying lesion within the spinal canal is observed.
II. Potential Diagnoses
Based on the imaging characteristics and case history, and given that this 48-year-old female patient currently has no known history of tumors or systemic disease, the possible diagnoses or differential diagnoses include:
- Benign Notochordal Cell Tumor (BNCT):
This type of lesion is often an incidental finding, typically showing low or isointense signal on T1WI and high signal on T2WI, without significant enhancement or soft tissue invasion. These features correspond to this case. - Chordoma:
Although also originating from notochordal remnants, chordomas usually exhibit more evident bone destruction, soft tissue masses, and noticeable enhancement. In this case, the absence of a clear soft tissue component argues against chordoma. - Metastatic Tumor:
Usually associated with a known cancer history or multifocal lesions, often accompanied by osteolytic changes or other destructive features. - Hemangioma:
Typically presents a “striped” appearance or noticeable vascular flow voids on MRI. On CT, it often appears as a low-density or mixed-density lesion, more commonly found in the thoracic or lumbar vertebrae. These features do not fully match this case.
III. Final Diagnosis
Considering the patient’s age, clinical symptoms (chronic back pain), lack of previous cancer history, and the typical MRI and CT features, the lesion is more likely to be diagnosed as a Benign Notochordal Cell Tumor (BNCT). Current studies suggest such lesions are benign and often do not require surgical intervention. However, because some literature indicates a possible connection to chordoma, regular imaging follow-up is recommended to rule out any progression or malignant transformation.
IV. Treatment Plan and Rehabilitation
- Treatment Strategy
- Conservative Management: For most BNCT patients without significant neurological compression or severe pain, a conservative approach may be chosen, including pain management (e.g., oral anti-inflammatory analgesics) and regular imaging follow-ups.
- Surgical Intervention: Biopsy or surgery should be considered only if there is rapid lesion growth, bone destruction, nerve compression, or strong imaging suspicion of malignant change.
- Rehabilitation / Exercise Prescription
- Individualized Exercise Program: Based on the patient’s back pain severity and physical condition, it is recommended to start with low-intensity, supported exercises, such as regular walking on flat ground or using the elliptical machine for about 15 minutes, 3–5 times per week.
-
FITT-VP Principle (Progressive Overload):
Frequency: Start with 3 sessions per week, then gradually increase to 5 times per week when pain improves;
Intensity: Mild sweating and a slightly elevated heart rate are acceptable. Avoid high-impact activities;
Time: Depending on the patient’s tolerance, gradually extend each session from 15 to 30 minutes;
Type: Focus on low-impact aerobic exercise, with moderate core stabilization training (e.g., planks);
Progression: If tolerable, incrementally increase exercise volume or duration every 2–4 weeks. - Precautions: Reduce exercise intensity and avoid weight-bearing or strenuous activities if back pain worsens. Seek medical advice promptly if new or worsening symptoms occur, especially neurological symptoms such as numbness or severe pain in the lower limbs.
Disclaimer
This report is based solely on the current imaging and clinical information and provides a reference analysis. It is not a substitute for an in-person evaluation or professional diagnosis by a physician. If you have further questions or if symptoms change, please seek medical attention and follow a specialist’s advice.
Human Doctor Final Diagnosis
Sacral benign notochordal cell tumour