Unilateral distal clavicular osteolysis in an amateur bodybuilder



Clinical History
A 29-year-old amateur bodybuilder is referred with right shoulder pain for two weeks, worsening during training. There is no history of trauma. The right shoulder shows a normal range of motion, but O'Brien's compression test is positive. There is tenderness upon palpitation of the acromioclavicular joint.
Imaging Findings
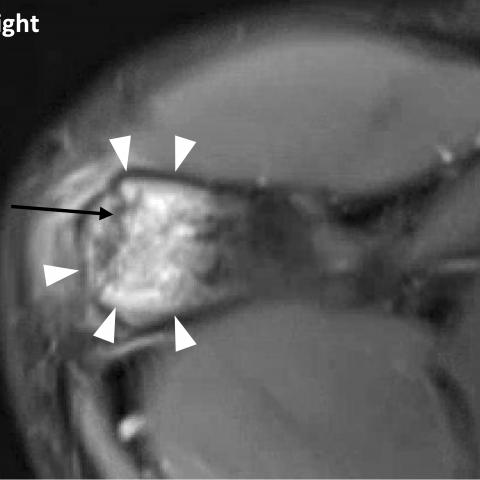
Digital radiograph and ultrasound of the shoulder are performed for a suspected rotator cuff tendinopathy. Periarticular osteopenia and cortical irregularity in the distal clavicle with a mild joint effusion in the acromioclavicular joint is found (Figs. 1a, 1b and 2). Subsequent magnetic resonance (MR)-imaging shows marked bone marrow oedema in the right distal clavicle with a hypertrophic acromioclavicular (AC) joint capsule (Fig. 3). Side-to-side comparison to the left confirms unilateral bone marrow oedema with bone erosions and subchondral cortical thinning of the pathological right side, thus confirming unilateral disease (Fig. 4a and 4b).
Discussion
Distal clavicular osteolysis (DCO) is a self-limiting pathology most caused by overuse injury. The pathogenesis is debated, but likely involves subchondral microfractures caused by repetitive activity with compression of the distal clavicle [1]. Stress-induced DCO is most often seen in weightlifters or athletes who are engaged in strenuous training of the upper extremity in which the AC-joint is subjected to forces as if it were a weight-bearing joint, sometimes leading to bilateral DCO [2]. DCO is also seen in overhead athletes and workers [3].
Clinical findings are non-specific and include tenderness to palpation of the AC-joint, elicited pain with cross-body adduction but a normal range of motion [4]. Patients complain of vague anterior shoulder girdle pain: increased at night following intense weightlifting during the day, relieved with decreased activity [5].
Digital radiographs are not sensitive to detect DCO in the early stage of the disease. Initial findings are subtle, such as periarticular osteopenia or loss of subchondral cortex. In the progressive lytic stage, cortical thinning, irregularity and erosions in the distal clavicula can be seen, while the acromial surface remains normal [5]. For early diagnosis, both MR-imaging and bone scintigraphy are far more sensitive. MR-imaging typically shows high signal intensity to muscle in the distal clavicle on T2- or PD-fat suppressed sequence, correlating with bone marrow oedema. This may also be present in the articular part of the acromion, but less pronounced [6]. Other MR findings include the same radiographic features, but also capsular thickening and joint effusion of the AC joint [6]. In the early stage, bone scintigraphy will demonstrate increased uptake in the distal clavicle, consistent with the theorized pathogenesis, visualizing increased osteoblast activity [5].
Initial treatment is mostly conservative, including activity modification and nonsteroidal anti-inflammatory drugs (NSAIDs), often successful after 3-6 months. Long-term sequelae on MRI include widening of the AC joint and AC joint osteoarthritis. In severe cases, resection of the distal clavicle has demonstrated acceptable clinical outcome [5, 6].
The radiologist should be aware that DCO affects a certain population such as weightlifters and should be included in the differential diagnosis in case of atraumatic shoulder pain. Key for the diagnosis are subtle changes on digital radiograph, which can be magnified by comparative incidences, followed by MRI or bone scintigraphy to confirm the diagnosis. Comparative MRI will be helpful to exclude bilateral DCO.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Unilateral distal clavicular osteolysis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures


Ultrasound of the right acromioclavicular joint

Fat-saturated coronal magnetic resonance protondensity-weighted images of the right acromioclavicular joint


Radiological Findings
Based on the provided imaging (including X-ray, MRI, and ultrasound) and in combination with the patient's complaints, the following main features can be observed:
- The cortical bone in the right distal clavicle is thinned and irregular, indicating mild osseous destruction or osteolytic-like changes locally.
- X-ray findings: Irregular cortex in the distal clavicle with slight widening of the articular space on the AC joint side, or relatively abnormal appearance compared to the unaffected side.
- On the MRI T2 or PD Fat-Suppression sequences, a hyperintense lesion is visible in the distal clavicle, suggesting local bone marrow edema; the joint capsule is thickened, and there is a small amount of effusion in the AC joint.
- Ultrasound also indicates erosive changes in the distal clavicle, with the joint space region (marked with an asterisk) showing unclear boundaries from the surrounding soft tissues, and a noticeable defect in the joint protrusion morphology.
Potential Diagnoses
- Distal Clavicular Osteolysis (DCO)
Cause: Commonly seen in individuals who engage in weightlifting or other physical training involving significant or repetitive shoulder loading. Continuous overtraining leads to repeated microfractures and an imbalance in bone repair at the distal clavicle, resulting in bone resorption.
Imaging Features: Erosive-like changes in the distal clavicle with bone marrow edema and joint capsule thickening. Often lacking a clear history of trauma, but physical exams may reveal tenderness over the AC joint and a positive O’Brien’s test. - AC Joint Osteoarthritis
Cause: Occurs with aging or prolonged wear-and-tear of the joint. It can share some imaging overlap with DCO, but degenerative changes often involve both the acromial and clavicular sides of the joint. - AC Joint Soft Tissue Injury or Subclinical Fracture
Cause: Any hidden trauma or excessive load can cause partial dislocation of the AC joint, cartilage injury, or microfractures. In most cases, imaging may show soft tissue swelling or more obvious joint displacement.
Final Diagnosis
Considering the patient’s age (29 years, male), gym training history, imaging findings (destructive changes in the distal clavicle, bone marrow edema, etc.), as well as local tenderness and a positive O’Brien’s sign, the most likely diagnosis is:
Distal Clavicular Osteolysis (DCO).
Treatment Plan and Rehabilitation Program
1. Treatment Strategies
- Conservative Treatment:
- Reduce or pause exercises that place excessive load on the shoulder joint (e.g., bench presses, overhead lifts) to decrease stress on the AC joint.
- Oral NSAIDs (non-steroidal anti-inflammatory drugs) to relieve pain and local inflammation.
- Local physical therapy (cold or heat therapy alternation) and rehabilitation exercises targeting the shoulder girdle muscles.
- Injection Therapy:
For prolonged symptoms that do not improve significantly with conservative treatment, consider intra-articular injections of corticosteroids or hyaluronic acid to reduce inflammatory responses. - Surgical Treatment:
For persistent symptoms that significantly affect daily function, partial resection of the distal clavicle (Mumford procedure) may be considered, often yielding good outcomes post-surgery.
2. Rehabilitation/Exercise Prescription Recommendations (FITT-VP Principle)
During conservative management or post-operative rehabilitation, exercises should be individualized and progressed gradually.
- Frequency:
Initially, specialized shoulder rehabilitation exercises are recommended 2–3 times per week, gradually increasing to 3–4 times depending on symptom relief. - Intensity:
Begin with low-intensity, low-load exercises, such as those using resistance bands or light dumbbells. Avoid movements that cause significant pain. - Time:
Each session should last about 15–30 minutes. As function improves, gradually extend to 30–45 minutes. - Type:
Isometric and isotonic resistance training for the shoulder girdle (e.g., internal/external rotation exercises), combined with scapular stabilization exercises (such as “Y-T-W” motions). - Progression:
Increase load or difficulty gradually as tolerated without exacerbating pain. Avoid sudden large increases in training volume that could trigger recurrent inflammation. - Volume:
Gradually increase the total training volume. Start with low weights for multiple repetitions (e.g., 10–15 reps per set, 2–3 sets), and increment over several weeks based on tolerance.
If the patient has other underlying conditions (e.g., osteoporosis, cardiopulmonary insufficiency), consultation with a physician or rehabilitation specialist is advised to avoid complications from overexertion.
Disclaimer: This report offers a reference-based medical analysis drawn from available case information and imaging data and is not a substitute for in-person consultation or professional medical advice. If you have further questions or your symptoms worsen, please seek medical attention promptly.
Human Doctor Final Diagnosis
Unilateral distal clavicular osteolysis