

A 16-years-old male with a history of non-Hodgkin lymphoma in remission for five years presented with a slowly growing and slightly painful mass in the posterior left arm.
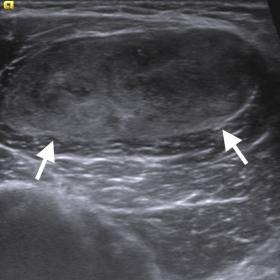
Grey-scale ultrasonography (US) demonstrated a well-defined, 5 cm solid mass in the triceps muscle with heterogeneous echotexture including isoechoic and hypoechoic areas. Colour flow Doppler US revealed mild vascularity within the mass (Figure 1).
The mass presented with the following imaging features on magnetic resonance imaging (MRI); isointense with skeletal muscle on T1-weighted (W); slightly heterogeneous and hyperintense on T2W images and almost homogenous enhancement in the delayed phase of the contrast administration (Fig.2, Fig.3). Dynamic contrast-enhanced (DCE) MRI revealed type III (rapid early enhancement followed by plateau/no significant wash-out) enhancement pattern an early enhancement noted within 7 s of contrast arrival into adjacent vascular structures (Fig.4).
In ADC maps, values varied between 0.9x10-3mm2/s and 1.7x10-3mm2/s (Figure 5).
Positron emission tomography revealed low uptake (SUV: 1) of 18F-Fluorodeoxyglucose in the mass with no metastasis in other sites of the body (Figure 6).
Synovial sarcoma (SS) is a malignant tumor arising from mesenchymal cells and assumed to have resulted from the presence of a t(X:18) translocation with a fusion of the SYT (at 18q11) and SSX1 or SSX2 genes (at Xp11) which is present in 95% of tumours [1]. SS accounts for 8% to 10% of all soft tissue sarcomas being second-most prevalent soft tissue tumours after rhabdomyosarcoma in children and adolescents [2].
Patients with SSs usually present with slowly enlarging mass with or without pain [2]. Extremities are the most frequent site (80% to 95%) of involvement [2]. On US, SSs may present as round or lobulated, solid, hypoechoic mass resembling a benign tumour but some may show a heterogeneous and complex echotexture including hypoechoic and hyperechoic areas with irregular margins [3]. On CT, SSs most commonly present as well-circumscribed and non-infiltrative deeply seated mass with slightly lower attenuation compared to skeletal muscle [1].
On MRI, SS typically appears as a prominently heterogeneous multilobulated soft tissue mass with signal intensity similar to or slightly higher than that of skeletal muscle on T1-weighted (T1W) MR images. In T2W images, lesions mostly demonstrate heterogeneous high signal intensity [1]. T2W images may demonstrate characteristic ‘triple signal intensity’ that refers to the combination of high, intermediate, and low signals in the mass representing areas of necrosis, calcification, haemorrhage, and cyst formation respectively [1, 4]. SSs usually shows diffusion restriction on DWI, it has been shown that ADC values may range between 0.8 – 1.9 x 10 -3 mm2/s [5, 6]. In our patient, ADC values ranged between 0.96 –1.68x10-3mm2/s.
Synovial sarcomas manifest with early diffuse enhancement at dynamic contrast-enhanced MR imaging [8]. It has been shown that rather than peripheral enhancement and washout phase enhancement of tumour, within 7 s after arterial enhancement is the only sign that occurs consistently in synovial sarcoma patients as seen in our patient [8].
Treatment of SS may be accomplished with surgery with or without
chemotherapy and/or radiotherapy. Tumours with high grade or large size (> 5 cm) or where resection is felt to be difficult and margins will be close or positive may need neoadjuvant chemotherapy followed by surgical excision [1].
Take-Home Message / Teaching Points:
Synovial sarcoma (monophasic type) in the triceps muscle
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.











This case involves a 16-year-old male with a progressively enlarging, mildly painful mass palpable in the posterior region of the left upper arm. Ultrasound (US) shows a relatively well-defined hypoechoic lesion with heterogeneous internal signals. Color Doppler reveals a certain degree of blood flow. MRI demonstrates a lesion with T1-weighted signal intensity similar to or slightly higher than skeletal muscle, high signal intensity on T2-weighted images (T2W), and areas of heterogeneous signals with septations or lobulations. Dynamic contrast enhancement shows rapid enhancement of the mass, with uniform or diffuse enhancement during the early arterial phase. DWI indicates restricted diffusion with relatively low ADC values (about 0.96 – 1.68×10-3 mm2/s), suggesting high cellular density. PET-CT shows moderate FDG uptake in the lesion. Overall, the imaging characteristics suggest a malignant lesion commonly seen in adolescent limb soft tissues.
Taking into account the patient’s history of non-Hodgkin lymphoma (remission for 5 years), current age of 16, a slowly enlarging mildly painful lesion in the posterior region of the left arm, MRI findings (high signal on T2W images, rapid enhancement, restricted diffusion), and pathological detection of the t(X;18) fusion gene, the most likely diagnosis is Synovial Sarcoma. If any clinical doubt remains, a biopsy or surgical pathology is recommended for further confirmation.
The rehabilitation program should consider the extent of surgery, the impact on joint mobility, and the patient’s overall physical condition. It should follow a gradual, individualized approach.
Safety Precaution: If radiotherapy or chemotherapy is administered concurrently, reduce exercise intensity to prevent excessive fatigue or compromised immune function. Regular blood tests and imaging follow-up are necessary.
Disclaimer: This report is for medical information reference only and cannot replace in-person consultation or personalized advice from a professional physician. The actual diagnosis and treatment plan should be determined by a specialist after comprehensive evaluation of the patient’s specific condition.
Synovial sarcoma (monophasic type) in the triceps muscle