Humeral hydatid cyst complicated with extraosseous involvement: a case of unusual location of echinococcosis



Clinical History
Previous 5 months: a painless, enlarging mass in the left arm. Physical examination: Tenderness and moderate powerloss of the left arm. The shoulder’s motion was limited in abduction. Imaging: Distortion of the axis and regional expansion of the humeral shaft with minimal thinning areas of the cortex. Polycystic appearance of the bone marrow with regional calcifications into the lumen and at the soft tissues of the upper arm. A large cystic lesion at the upper arm with some foci of calcifications. 99mTc-DMP scintigraphy showed significant deposition of the radionuclide at the distal part of the left humerus and elbow as well as a smaller deposition foci at the upper 1/3 of it.
Imaging Findings
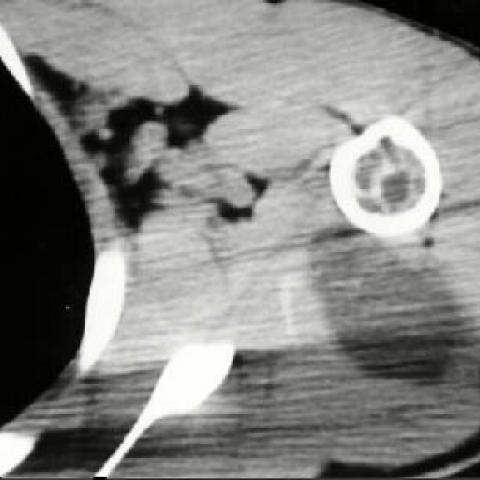
A 17-year-old male was admitted to hospital with a five months history of a painless, enlarging mass in the left arm. He had no fever, chills, weight loss or prior trauma. Physical examination revealed tenderness and moderate powerloss. The shoulder’s motion was limited in abduction. Plain film of the left humerus demonstrated distortion of the axis, regional expansion of the humeral shaft with minimal thinning areas of the cortex. Additionally, numerous radiolucent areas of the humeral shaft were observed especially at the distal part of the bone. No calcification of the soft tissues was noticed (figure 1a,1b). Computed tomography examination showed significant destruction of the trabecular bone of the humeral head and polycystic appearance of the bone marrow with regional calcifications into the lumen. Additionally, a large cystic lesion between medial and lateral head of the triceps muscle with some foci of calcifications were observed (figure 2a,2b). Magnetic resonance imaging revealed the multilocular nature of the lesion into the humeral lumen with a cystic lesion involving the soft tissues of the upper arm. The cyst showed contrast enhancement at the pericyst capsule of the cyst after Magnevist administration (image 4a,4b) . 99mTc-DMP scintigraphy showed significant deposition of the radionuclide at the distal part of the left humerus and elbow as well as a smaller deposition foci at the upper 1/3 of it (figure 3).
Discussion
Hydatid disease, also referred to as ‘‘echinococcosis’’, is a parasitic disease most commonly caused by Echinococcus granulosus that seldom involves the skeleton and is still common in the countries of the temperate zones. Skeletal involvement by Echinococcus granulosus is a rare localization of echinococcosis since it occurs in only 0.28-3.1 % of hydatid disease cases. Moreover, humeral involvement is extremly rare, to our knowledge, only two cases are reported in the literature. CT and MRI examinations of our case determined the extent of the lesion, the relation to the normal tissues, and the preoperative planning of the surgical approach. The CT examination provided a precise assessment of the osseous part of the lesion, the extension into the soft tissues, and the calcifications into the humeral lumen. The MR imaging with the capability of demonstrating a very evocative cyst images, is the exam of choice in order to appreciate the disease’s extent and the degree of medular sufferance. Moreover, MR imaging is very useful in determining the extent of surgery. Our patient’s physical examination and X-ray features did not give any clues as to the possible diagnosis. However, CT and MRI examination displayed the multicystic appearance of the lesion at the humeral diaphysis as well as at the soft tissues of the upper arm but with no other specific and characteristic feature of hydatidosis such as the «water-lily» sign. Preoperative recognition of this rare entity is clearly difficult, particularly since all of the clinical signs of acute inflammation are absent. The purpose of the present study is to alert the reader to this rare entity so that open and percutaneous needle biopsies will be avoided. Furthermore, humeral or other long bone Echinococcus infestation may mimic a neoplastic process, leading to misdiagnosis. In conclusion, preoperative differential diagnosis of humeral cystic lesions should include hydatid disease, especially in endemic and sporadic echinococcosis areas, since it may easily be missed unless kept in mind. MRI is the method of choice for evaluation, preoperative planning of the surgical approach, and correct diagnosis of such lesions.
Differential Diagnosis List
Final Diagnosis
Humeral hydatid cyst complicated with extraosseous involvement: a case of unusual location of echinococcosis
Liscense
Figures
Plain film of the left humerus


Computed tomography examination

99mTc-DMP scintigraphy

Magnetic Resonance examination


99mTc-DMP scintigraphy

Medical Imaging Analysis Report
I. Imaging Findings
1. The provided X-ray reveals a certain degree of distortion along the left humeral shaft axis, with local bone expansion and cortical thinning, but no significant cortical discontinuity is observed. The medullary cavity shows multiple cystic-like changes, and small calcifications can be seen locally.
2. CT imaging demonstrates multiple cystic lesions within the humeral medullary cavity, some of which exhibit ring-like or spotted calcifications; a cystic shadow is also visible in the surrounding soft tissue. Although the bone cortex is thinned, there is no obvious fracture line.
3. MRI shows multiple cystic high T2 signal lesions in the humeral shaft and surrounding soft tissue, presenting septations or multiloculated features. Some lesions display thickened or calcified cyst walls. No extensive tumor-like soft tissue components within the bone marrow are noted.
4. 99mTc-DMP Bone Scan shows pronounced radiotracer uptake around the distal left humerus and elbow region, with a smaller uptake area in the proximal humerus, suggesting active lesions in those regions.
II. Potential Diagnoses
Based on multifaceted cystic bone lesions, local calcification, and the potential epidemiological background (such as a possible parasite-endemic region), the following conditions are considered:
1. Hydatid Disease of the Bone (Echinococcosis): Involving long bones such as the humerus, it often presents as multicystic bone destruction, typically appearing “honeycombed” or “multi-cavitated,” sometimes with calcifications. As the parasite grows within the bone, it can cause extensive bone destruction.
2. Aneurysmal Bone Cyst (ABC): Usually demonstrates expansile, septated bone destruction and may show fluid-fluid levels, although prominent calcifications are uncommon. Often accompanied by pain or pronounced local swelling.
3. Simple Bone Cyst: Common in adolescents, can be unilocular or occasionally multilocular, but typically lacks calcified cyst walls.
4. Bone Tumors (e.g., Chondrosarcoma, Giant Cell Tumor of Bone, etc.): Some may display multicystic or septated destructive lesions with calcification. However, they usually show significant cortical destruction or more typical cartilaginous matrix/soft tissue masses on imaging.
III. Final Diagnosis
Taking into account the patient’s age, medical history (no significant pain, but a progressively enlarging mass), epidemiological background (possibility of parasitic infection even in temperate regions), and the multi-cystic lesions with calcification on CT/MRI, the most likely diagnosis is Hydatid Disease of the humerus (Echinococcosis).
For definitive confirmation, serological tests (e.g., Echinococcus antibody testing) and pathological examination can be considered. In clinical practice, if hydatid disease is strongly suspected, caution should be exercised to avoid open or needle biopsy to prevent leakage of cyst fluid and possible dissemination.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy:
- Surgical Treatment: Given the extensive lesion and significant local bone destruction, a complete surgical excision or thorough curettage is generally recommended along with meticulous measures to prevent spread (e.g., irrigating with antiparasitic solutions). If necessary, bone grafting, internal fixation, or bone cement might be used to reconstruct the humeral structure.
- Medication: For bone hydatid disease, antiparasitic agents (such as albendazole) are usually administered before and after surgery to reduce recurrence and control residual lesions.
- Other Supportive Care: Standard postoperative analgesia, infection prevention, and close monitoring of hematologic and immune parameters should be undertaken, with regular follow-up appointments.
2. Rehabilitation and Exercise Prescription:
- Early Postoperative Phase (Weeks 1-4):
· Focus on protective immobilization and isometric muscle exercises, maintaining a limited range of motion in the shoulder and elbow joints, avoiding weight-bearing and excessive movement.
· Low-intensity isometric muscle training can be performed 2-3 times a day, each session lasting 10-15 minutes, ensuring pain is not exacerbated by the exercises.
- Mid Postoperative Phase (Weeks 4-8):
· Gradually increase the range of motion of the shoulder and elbow joints under professional guidance, introducing light resistance training.
· Apply the “FITT-VP” principle: exercise 3-4 times a week, progress from low to moderate intensity, 20-30 minutes per session, adjusting modes of exercise as necessary.
- Late Postoperative Phase (Week 8 and Beyond):
· Once bone healing and local pain are well controlled, begin functional upper limb strength and proprioceptive training to gradually return to daily and sports activities.
· Progressively load the limb; avoid premature overuse to reduce the risk of reinjury.
- Individualized Approach:
· For patients with weakened bone or other comorbidities (e.g., compromised cardiopulmonary function), reduce exercise intensity and shorten each training session, distributing activities across multiple sessions.
· The entire rehabilitation process must be coordinated with specialists and rehabilitation therapists, adjusting the plan based on bone healing and symptom changes.
V. Disclaimer
This report is solely a reference based on current information and cannot replace in-person consultations or the official medical opinion of a professional physician. Specific clinical diagnosis and surgical decisions should be made upon comprehensive assessment by qualified medical personnel, considering each patient’s actual situation.
Human Doctor Final Diagnosis
Humeral hydatid cyst complicated with extraosseous involvement: a case of unusual location of echinococcosis