Bilateral ischial apophysitis in a football player



Clinical History
An adolescent male, 14-year-old, and a member of a private football academy, presented with pain at his sitting bones. The pain was initially related to training and then became persistent all the time and manifested severely while sitting, standing, and kicking. He had to suspend training and seek medical advice. At clinical examination, exquisite pain was limiting active hip flexion and extension. The maximum point of tenderness was at pressing on sitting bones. No muscle wasting, leg deformity or gait abnormality. Neurological examination was free.
Imaging Findings
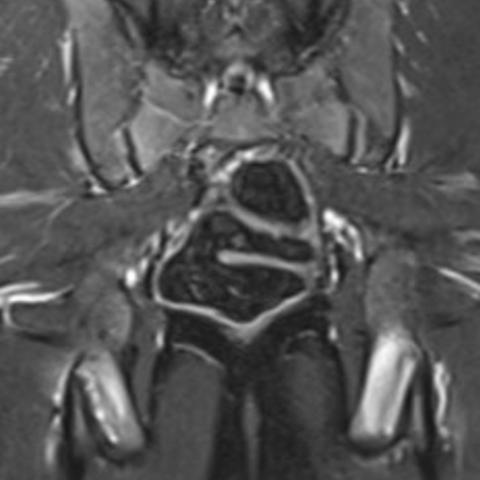
Plain X-ray of the pelvis demonstrated bilateral irregular cortical margins of the ischial tuberosities with no definite displaced avulsed bone fragments (Figure 1a and 1b). Magnetic Resonance Images (MRI) revealed bilateral symmetrical ischial tuberosity bone oedema associated with intrasubstance oedema at the hamstring tendon origin (Figure 2a and 2b).
Discussion
An apophysis is the anatomical site of a tendon attachment to bone in the skeletally immature. The ischial tuberosity apophysis hosts the hamstring tendons attachment. Ossification starts to appears after the age of 10 years in girls and 11 years in boys, with complete fusion is observed at the age of 16.9 and 17.8 years old in girls and boys respectively [1].
Sports injuries at the ischial tuberosity apophysis are common especially in football players. Acute avulsion injuries are the most encountered type of injury and are commonly described in literature in its acute and chronic clinical presentations [2–5].
Ischial apophysitis is a description of a clinical condition in which there is painful ischial apophysis in absence of avulsion. It is more common in athletes secondary to continuous tendon traction on growing bone and cartilage implying a form of stress and repeated microtrauma [2, 6]. The underlying pathogenesis is osteochondrosis, which is basically a disorder of growing cartilage at the long bone physeal growth plate, epiphyses or apophyses. It is of uncertain aetiology, but several factors have been suggested including vascular, hormonal, genetic factors. There is a strong association with the increased physical activities in adolescents and hence more common incidence among athletes [7]. Apophyseal osteochondrosis is commonly seen at the tibial tuberosity, “Osgood Schlatter disease” and also at the calcaneum, “Sever disease”. The incidence of ischial apophysitis is unknown. Few case reports are published [8–11].
Pelvis radiographs may be inconclusive. Asymmetrical appearance of the apophyses compared to the normal side may be helpful at showing some widening, sclerosis, cortical irregularity. MRI is the best imaging investigation to diagnose this condition, exploiting oedema at the anatomical site of tendon attachment, with the superior ability to show any tendon damage like degeneration or tear. It is important to differentiate these findings from the more common avulsion injury pattern which is usually an acute injury having a bone fragment is displaced from the original bone. Computed tomography (CT) would show irregular margins and possible fragmentation of the apophyseal margins. However, it is better to avoid unnecessary exposure in such age groups. Bone scintigraphy may show locally increased tracer uptake.
The diagnosis of ischial apophysitis implies rest and rehabilitation. In most cases, the condition is self-limiting and no intervention is required [6, 8].
Differential Diagnosis List
Final Diagnosis
Bilateral ischial apophysitis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures




1. Imaging Findings
Based on the anteroposterior (AP) X-ray of the pelvis, both ischial tuberosities appear generally normal in shape, with no clear detached bone fragments observed. However, the affected side (right or left) may show slight sclerosis, irregular edges, or mild bulging of the ischial tuberosity when compared to the unaffected side.
MRI (T2-weighted or STIR sequence) shows enhanced signals around the tendon attachment of the ischial tuberosity, indicating localized edema. The tendon itself does not exhibit obvious signs of rupture, and the cortical bone continuity is largely preserved without a clear fracture line. Overall, the imaging characteristics suggest inflammation or mild changes at the ischial tuberosity attachment site, presenting primarily as edema and subtle morphological abnormalities.
2. Possible Diagnoses
- Ischial Tuberosity Avulsion Fracture: Commonly seen in acute injuries due to intense physical activity or sudden muscle contraction. Radiologically, there would typically be a noticeable detached fragment or bone fragment. In this case, there is no obvious separation of bone fragments, making an acute avulsion fracture less likely.
- Hamstring Tendinitis/Tendinopathy (Proximal Hamstring Tendinopathy): Often associated with overuse injuries, it can present with tendon edema and abnormal signal changes. However, in adolescents whose growth plates or ossification centers have not fully fused, apophyseal issues should be closely monitored.
- Ischial Apophysitis (Inflammation of the Ischial Apophysis): Common in adolescent athletes, caused by repeated traction and microtrauma at the ischial apophysis and adjacent cartilage. X-ray findings can be subtle, and MRI typically demonstrates edema in the apophysis and surrounding soft tissues.
3. Final Diagnosis
Considering the patient’s age (14 years old), clinical symptoms (pain at the ischial tuberosity aggravated by activities), and imaging findings (MRI shows local edema at the ischial tuberosity without obvious avulsion or fracture line), the most likely diagnosis is:
Ischial Apophysitis.
4. Treatment Plan and Rehabilitation
Management of ischial apophysitis generally involves conservative treatment, combined with a gradual rehabilitation and training program:
- Rest and Avoidance of Excessive Weight-Bearing: Advise reducing or temporarily stopping high-intensity training (e.g., kicking motion in soccer, jumping, or vigorous hip extension) to allow the apophysis sufficient time to reduce inflammation.
- Physical Therapy and Anti-Inflammatory Measures: Nonsteroidal anti-inflammatory drugs (NSAIDs) or local therapies (e.g., heat, ultrasound) may be used to relieve pain and inflammation. Manual therapy may also help release muscle tension.
- Strength and Flexibility Training:
- Stage 1: Perform gentle lower limb and hip mobility exercises within pain tolerance, focusing on mild static stretches (for example, the hamstrings and quadriceps), avoiding aggressive stretching.
- Stage 2: After significant pain relief, gradually introduce core strengthening exercises and lower limb strength training, such as bridge exercises or small-range lunges, avoiding excessive tension or load on the ischial tuberosity.
- Stage 3: Progress to light plyometric and sports-specific drills (e.g., low-intensity ball juggling or slow, short-distance dribbling), while closely monitoring pain.
- Gradual Return to Sports (FITT-VP Principle):
- Frequency: 3–5 times per week, based on recovery status.
- Intensity: Start at a low intensity, avoiding any movement that triggers significant pain.
- Time: Begin with about 15 minutes per session, gradually increasing to 30–45 minutes.
- Type: Focus on low-impact strength and flexibility exercises, gradually transitioning to soccer-specific drills.
- Progression: Adjust according to pain or fatigue levels. If pain recurs, revert to the previous stage or pause temporarily.
- Preventing Re-Injury: During subsequent training and competitions, prioritize preemptive stretching and proper warm-up for the hip, pelvis, and hamstring muscles.
Disclaimer: This report is based on the provided information for reference only and does not replace an in-person consultation or professional medical advice. If symptoms worsen or in case of any emergency, please seek medical attention promptly.
Human Doctor Final Diagnosis
Bilateral ischial apophysitis