Extrahepatic metastases from hepatocellular carcinoma



Clinical History
A patient with hepatocellular carcinoma was treated with transcatheter arterial chemoembolisation. One year later he reported a sore solid mass at the right shoulder.
Imaging Findings
The patient, affected with chronic hepatopathy and hepatitis C, presented with a hepatocellular carcinoma (HCC) nodule in the seventh hepatic segment. He was treated with transcatheter arterial chemoembolisation (TACE) and subjected to CT follow up.
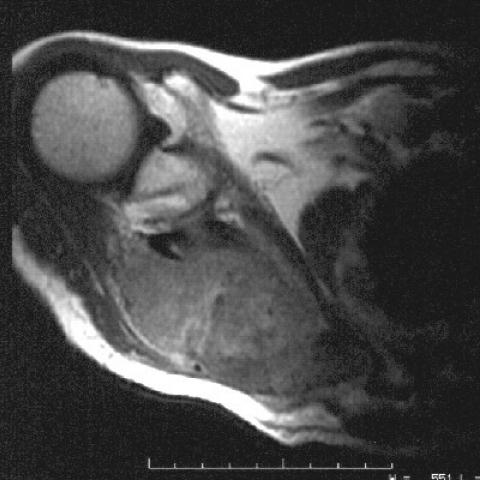
One year later he reported a sore solid mass at the right shoulder. US and MRI were performed, showing a metastasis from the HCC to the shoulder blade.
Discussion
HCC is an aggressive tumour with different treatment options depending on the stage of the tumour. The incidence of HCC is increasing, not only in Japan but also in the United States, because of an increased rate of viral hepatitis, in particular from previously undiagnosed hepatitis C. An incidental extrahepatic lesion discovered at imaging in a patient with HCC may in fact be benign. If such lesions are assumed to be malignant, curative surgical therapies such as orthotopic liver transplant or resection may not be offerd and the patient will be left with only palliation. In both clinical settings, knowledge of the local and radiographic appearances of metastatic HCC is important in assuring the patient the most appropriate therapy and the best chance of survival.
Bone metastases from HCC are fairly rare, their average occurence rate being 7.3%. All bone metastases are lytic and involve the lumbosacral or the thoracic spine; more rarely, at initial presentation, some patients have rib lesions, or lytic lesions of the lumen acetabulum or ilium and lytic destruction of the sternum, shoulder blade or femur. The meatstases are demonstrated by radiography, CT, and nuclear scintigraphy, in patients with skeletal pain; CT scans demonstrate the destructive nature of the lesions, which are associated with bulky soft-tissue masses.
The authors believe that bone scintigraphy should be included in the staging protocols of the HCCs which need a potentially curative therapy. Bone metastases are frequently detected in the early stages of cirrhosis and HCC, which suggests that patients might experience long survival if adequately treated with radio-chemotherapy.
Differential Diagnosis List
Final Diagnosis
Metastatic bone disease from hepatocellular carcinoma
Liscense
Figures
MR examination


Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided cross-sectional MRI images, a soft-tissue mass or space-occupying lesion is observed in the right shoulder region (including the shoulder joint and surrounding soft tissues). The lesion presents a marked abnormal soft-tissue density/signal that may involve the local bone structure. Given the anatomical complexity of this area, the lesion is closely adjacent to the surrounding muscles and joint capsule. Specific features include:
- The lesion is located near the right shoulder joint, showing a soft-tissue swelling or mass with an ill-defined boundary.
- The local bone may display uneven signals, suggesting potential bony destruction or cortical involvement (further confirmation needed).
- There may be enhancement or necrotic areas within or around the soft-tissue lesion, requiring contrast-enhanced sequences and other imaging planes to confirm.
- The overall lesion signal significantly differs from the surrounding shoulder muscle tissue, indicating space-occupying characteristics.
II. Potential Diagnoses
Considering the patient's basic clinical history (hepatocellular carcinoma, previously treated with transcatheter arterial chemoembolization), the following possibilities should be considered for the soft-tissue mass or destructive bony lesion in the shoulder:
- Hepatocellular carcinoma (HCC) bone metastasis: Although bone metastasis is relatively uncommon in HCC, it must be taken into account in advanced or recurrent cases. For lesions with obvious soft-tissue masses, bone destruction, and pain, bone metastasis is the primary differential diagnosis.
- Primary bone or soft-tissue sarcoma: If the lesion is not directly related to the existing HCC, it could be a primary sarcoma in the shoulder/proximal humerus region, such as osteosarcoma or soft-tissue sarcoma. These tumors can manifest as aggressive destruction and mass formation.
- Other metastatic tumors: If the patient has multiple lesions or any other tumors, metastasis from another primary site should be ruled out, especially when encountering a single focal destructive lesion.
- Benign or subacute lesions (e.g., giant cell tumor of bone, aneurysmal bone cyst, etc.): Although less common than malignant lesions, benign tumors or cystic lesions in the shoulder area must also be excluded. However, given the clinical context here, a benign lesion is less likely.
III. Final Diagnosis
In light of the patient's age (76 years), history of hepatocellular carcinoma, and the aggressive bone or soft-tissue lesion appearance on MRI accompanied by local shoulder pain, the most likely diagnosis is:
“Hepatocellular carcinoma bone metastasis (involving the right shoulder bone and soft tissues)”
Further diagnostic confirmation is recommended through:
- Evaluating serum tumor markers (e.g., AFP).
- Contrast-enhanced MRI or CT of the shoulder to determine lesion extent.
- Bone scan (or PET-CT) to assess for systemic skeletal metastases.
- Biopsy to obtain histological evidence confirming whether the lesion is an HCC metastasis.
IV. Treatment Plan and Rehabilitation
- Treatment Strategy:
- Tumor-specific management: If confirmed as HCC bone metastasis, consider local radiotherapy, palliative resection, or combined radiochemotherapy to relieve pain and control local progression.
- Systemic therapy: Continue assessing the liver condition, and consider combining HCC-targeted therapies, immunotherapy, or other systemic chemotherapy as needed.
- Supportive therapy: Pain management (oral or topical analgesics) and bone-protective agents (bisphosphonates or osteoclast inhibitors) to prevent further bone destruction or fracture.
- Surgical indications: If there is significant local pain or a high risk of bone destruction, surgical fixation or decompression may be considered to prevent pathological fracture and improve quality of life.
- Rehabilitation/Exercise Prescription (Gradual Progression):
- Within the tolerable range of pain and bone stability, gentle shoulder and upper limb activities such as pendulum exercises and assisted stretching are recommended to maintain joint mobility.
- Initial stage: 2–3 times per week, 10–15 minutes per session of light upper limb stretching and range-of-motion exercises, avoiding excessive load.
- Intermediate stage: When symptoms are stable and approved by a physician, gradually increase to 20–30 minutes per session, with low-resistance exercises using resistance bands. Movements should be slow and avoid exacerbating pain.
- Later stage: If the lesion is effectively controlled or upon clearance by a physician and rehabilitation specialist, progressively add strength training with small weights (1–2 kg) or machine-assisted workouts, 3–4 times per week.
- Throughout, closely monitor pain, fatigue, and bone stability. If marked discomfort (increased pain, joint swelling, limited mobility) occurs, seek medical advice promptly.
- Precautions:
- Patients with bone metastases should be alert to the risk of pathological fractures; proper safety and correct posture are crucial during exercise.
- If there is compromised cardiopulmonary or liver function, consult relevant specialists before creating an individualized exercise plan.
- Physical therapy, nutritional support, and psychological counseling are recommended throughout to improve treatment outcomes and quality of life.
V. Disclaimer
This report provides a preliminary medical analysis based on the provided information and is for reference only. It cannot replace an in-person consultation or professional medical advice. If you have any questions or if your symptoms worsen, please consult a specialist or visit a hospital promptly.
Human Doctor Final Diagnosis
Metastatic bone disease from hepatocellular carcinoma