Posterior Interosseous Nerve Entrapment-an uncommon entity



Clinical History
A 13 years-old female was referred to the plastic surgery for a left-hand deformity characterized by persistent flexion of the index through small digits, and persistent flexion of the wrist with ulnar deviation. There was no history of trauma, infection, or neuromuscular disorders. The patient's mother underwent an uncomplicated pregnancy, labor, and delivery.
Imaging Findings
Dedicated T1 weighted MRI imaging of the left forearm revealed marked atrophy within the extensor forearm muscles predominantly involving the extensor pollicis longus, extensor digiti minimi, extensor carpi ulnaris, and extensor digitorum. No associated fatty infiltration and lack of muscle oedema to suggest a longstanding process (Fig.1a,b,c).
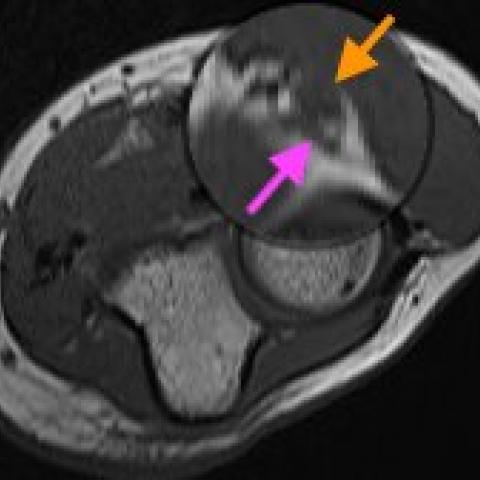
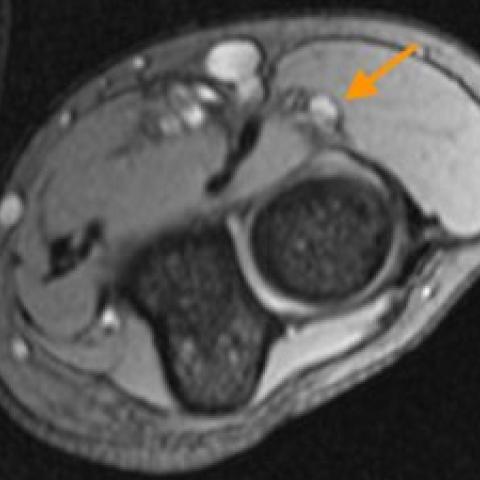
In addition, there was a focal lesion/fusiform thickening measuring 4 x 3 mm of the posterior intraosseous nerve (PIN), deep to the brachioradialis muscle belly and proximal to the supinator muscle. The thickening appeared isointense to the muscle on T1 weighted imaging, hyperintense on T2 weighted and gradient recovery sequences, without evidence of blooming (Fig.2 and 3). The radial nerve proximal to the elbow and its superficial branches appeared normal.
Based on the above MR findings, the reporting radiologist raised the possibility of a neurogenic tumour versus focal nerve thickening of posterior interosseus nerve secondary to a fibrous band with concurrent atrophy of extensor forearm musculature. Patient subsequently underwent decompression of the left PIN and nerve graft/transfer of the supinator branch to PIN. Intraoperatively the PIN was bulbous in shape with glassy washout appearance and was compressed at the level of the two heads of supinator/arcade of Frohse. No neurogenic tumor was identified.
Discussion
Entrapment of the PIN represents a rare neuropathy with an incidence of 0.03%, with a paucity of literature reported in the pediatric population (1). To our knowledge this case represents the first reported case of PIN entrapment secondary to the ligament of Frohse in a pediatric patient.
The two forearm supinator muscle layers, superficial and deep, form the supinator canal along the lateral antebrachial region, just distal to the cubital fossa. The posterior interosseous nerve, which branches from the radial nerve, passes through the supinator canal. The superficial layer of the supinator muscle forms the entrance of the supinator canal. A fibrous semicircular arch can be formed at the entrance of the supinator canal, which is known as the "arcade of Frohse" (2,3).
The most common cause of entrapment of the PIN is at the level of arcade of Frohse (4). Clinically, compression of the PIN can manifest with inability to extend the metacarpophalangeal joints of the finger and thumb, and weakness of thumb extension at the interphalangeal joint. Wrist extension is usually preserved due to radial nerve innervation of the extensor carpi radialis longus proximal to the terminal branch. Sensory manifestations include pain and decreased sensation overlying the radial and dorsal aspect of hand (4,5).
The arcade of Frohse can be identified on MRI as a hypointense band at the proximal edge of the supinator. Diagnosis of entrapment on MRI can be challenging given the small size of the PIN and arcade of Frohse. Often, muscle atrophy in the distribution of the PIN (abductor pollicis longus, extensor carpi ulnaris, extensor digiti minimi, extensor digitorum, extensor indicis, extensor pollicis brevis, and extensor pollicis longus) are the most apparent findings (2,7). As with other nerve entrapments, on MRI, the PIN can demonstrate focal fusiform/ nodular thickening, bright T2 weighted signal and occasionally, contact with the fibrous band of the ligament of Frohse if identified (2,3,7).
In our case, the ligament of Frohse is visible, however, it appears thin compared to the ligament of Frohse in adults(7). This may suggest that in pediatric patients with features of PIN entrapment, the ligament of Frohse may not always appear as an obvious band, and a thin hypointense band contacting the PIN should raise the possibility of fibrous entrapment by the ligament of Frohse. At the patient's first postoperative clinical visit, their weakness had not resolved, expectedly given the chronicity of the patient's symptoms. Physiotherapy and a follow-up clinic visit was planned for a later date.
Differential Diagnosis List
Final Diagnosis
PIN entrapment from ligament of Frohse
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures







Imaging Findings
- On MRI transverse images, a low-signal band can be observed near the lateral side of the proximal forearm close to the elbow, located at the edge of the shallow radial-side proximal supinator muscle. This band is close in position to the posterior interosseous nerve (PIN).
- When the posterior interosseous nerve enters the supinator canal, mild thickening/deformation of the local nerve fibers can be observed (with increased signal on T2-weighted sequences), suggesting possible compression or inflammatory changes.
- The fibrous band (Frohse ligament) does not appear significantly thickened on imaging, yet it is still seen in close contact with the posterior interosseous nerve.
- No significant muscle signal atrophy is noted in parts of the hand’s extensor muscle group (e.g., extensor digitorum communis, extensor digiti minimi, extensor pollicis brevis, etc.). However, as clinical symptoms have been chronic, the possibility of later denervation changes should be kept in mind.
Potential Diagnoses
- Posterior Interosseous Nerve (PIN) Compression Syndrome
Imaging findings suggest compression around the Frohse ligament, which aligns with a common mechanism of posterior interosseous nerve syndrome. Clinically, it may present as weakened finger joint extension, along with ulnar deviation of the wrist in some cases. Although rare in pediatric patients, this case aligns with the etiology and clinical manifestations reported in the literature. - Radial Nerve Trunk Lesion
If the site of compression were more proximal or involved the overall radial nerve trunk, symptoms such as inability to extend the hand or wrist drop might be observed. However, in this case, the primary issue is focused on the muscle group innervated by the posterior interosseous nerve, and some wrist extension function is preserved, making this less likely overall. - Idiopathic or Congenital Tendon-Muscle Abnormalities
Clinically, one must also rule out local tendon or muscle developmental anomalies when only considering symptoms. However, imaging does not suggest any obvious tendon or muscular structural abnormalities, so this is not a primary consideration.
Final Diagnosis
Based on the patient’s age, clinical presentation (limitations in finger and partial wrist extension), and MRI findings (indicating posterior interosseous nerve compression by the Frohse ligament), along with the relevant anatomical features, the most likely diagnosis is: Posterior Interosseous Nerve Compression Syndrome (caused by the Frohse ligament).
Treatment Plan and Rehabilitation
- Treatment Strategy:
- Conservative Treatment: For relatively mild or early-stage symptoms, try immobilization, avoid excessive forearm rotation and wrist movement, and use anti-inflammatory or analgesic medications or local injections for symptomatic relief.
- Surgical Indication: If symptoms significantly affect daily functioning or do not improve with conservative treatment, consider surgical release of the Frohse ligament to decompress the posterior interosseous nerve.
- After surgery, procedures such as nerve electrical stimulation and physical therapy can be employed to facilitate rapid recovery of nerve function.
- Rehabilitation and Exercise Prescription:
- Rehabilitation Principles: Gradual progression, individualized programs, and emphasis on safety. Avoid excessive stretching of the supinator muscle and protect the nerve pathway. Protect the surgical site if the patient undergoes surgery.
- Early Stage (Postoperative or Conservative Phase):
- Gentle fist making and finger extension exercises: 2–3 times daily, 10–15 repetitions each time, performing movements slowly and holding for 2–3 seconds.
- Active or passive wrist flexion and extension: 2–3 times daily, 10–15 repetitions each time, combined with gentle massage to promote blood circulation.
- Intermediate Stage (Strength and Nerve Function Recovery):
- Use elastic bands to strengthen the forearm’s extensor and flexor groups: 3 times per week, 2–3 sets each time, 10 repetitions per set, adjusting resistance according to tolerance.
- Fine motor skill training of the hand: Practicing tasks like picking up small beans and grasping small balls to enhance proprioception and nerve coordination.
- Late Stage (Return to Daily and Sports Activities):
- Gradually increase load and range of motion, such as using light dumbbells or resistance training 3–4 times per week, ensuring correct movement and posture.
- For patients with sports-related needs, progressive strength and coordination training under the guidance of a rehabilitation specialist or coach.
Disclaimer
This report provides a reference analysis based on existing imaging and clinical information and cannot replace an in-person consultation or professional medical opinion. In case of any questions or changes in symptoms, please seek medical attention promptly for a personalized and authoritative treatment plan.
Human Doctor Final Diagnosis
PIN entrapment from ligament of Frohse