Sacral insufficiency fracture



Clinical History
Four day history of severe lower back pain, exacerbated by movement. There was no history of trauma.
Imaging Findings
The patient, with a history of rheumatoid arthritis, was admitted with a four day history of worsening severe low back pain, exacerbated by walking. There was no history of trauma or previous back problems. She had previously been taking low dose corticosteroids. There was some tenderness at the lower back and sacrum, examination was otherwise unremarkable. There was no radiation of pain and no radicular symptoms or signs.
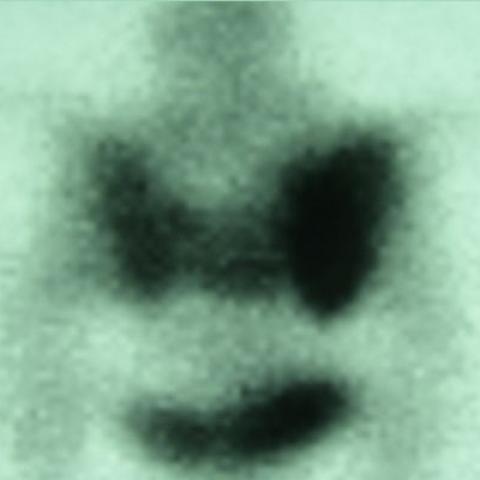
Plain radiographs (Fig. 1) were normal. MR imaging demonstrated low T1/high T2 signal intensity in both sacral alae, with enhancement after IV gadolinium chelate (Fig. 2 and 3). On bone scintigraphy there was increased isotope uptake throughout the sacrum, especially in the lateral masses, more marked on the right, with an ‘H’ shape (Fig. 4). CT scanning revealed bilateral sacral alae fractures parallel to the sacro-iliac joints (Fig. 5).
Based upon the clinical features and the imaging findings a diagnosis of bilateral sacral insufficiency fracture was made. Conservative treatment resulted in slow improvement and the patient has returned to normal activities. Follow-up CT scan showed sclerosis from fracture healing with no other abnormality.
Discussion
Elderly patients often present with low back pain and related symptoms. The features are often not specific and there are many possible differential diagnoses including malignancy, osteomyelitis and referred pain due to abdominopelvic diseases. Insufficiency fractures involving the sacrum are becoming acknowledged as an important and treatable cause. They need not be associated with trauma, are often difficult to identify and may mimic other conditions such as osteomyelitis, or malignancy, even on imaging. The potential to misinterpret is important as there is often a history of prior malignancy in the at-risk patient.
There are several associated risk factors, the commonest being osteoporosis. Patients with rheumatoid arthritis or on corticosteroid therapy are at risk, possibly because of osteoporosis. Other risk factors include pelvic irradiation and conditions that weaken bone such as osteomalacia, Paget’s disease, osteogenesis imperfecta, osteopetrosis and fibrous dysplasia, or according to one group, large Tarlov cysts.
These fractures are often bilateral and occur mostly in the sacral alae (lateral masses), paralleling the sacro-iliac joints. The sacral bodies may be involved. Their imaging features vary depending on the duration and the degree of healing.
Plain radiographs are generally non-contributory. MRI demonstrates low signal intensity on T1-weighted images and high signal intensity on T2-weighted images due to oedema within the bone marrow of the sacral ala. T2-weighted short tau inversion recovery (STIR) images are particularly sensitive. The fracture line is sometimes seen, but this is not usual. MR is sensitive, but usually non-specific and there may be enhancement after IV gadolinium chelate and the fracture may involve one or more sacral bodies. There is a potential to misinterpret as metastasis, especially if there is a previous history of malignancy.
Bone Scintigraphy is sensitive for suspected insufficiency fractures of the sacrum and the sacrum is best imaged on posterior views. Because the lateral masses are usually the site of these fractures and the sacral bodies are relatively spared, the isotope uptake classically produces a butterfly or ‘H’ pattern, which is considered diagnostic in the right setting. However, the fracture may be unilateral, with or without a horizontal bar to the ‘H’ and there may be extension into the iliac crest and other pelvic fractures and the classic ‘H-sign’ may only be seen in as few as 40% of cases, limiting specificity. The H-sign may be asymmetric as in the case presented.
CT is accurate, efficient and specific for diagnosing these fractures. It is helpful in confirming the diagnosis and excluding other pathology, after equivocal scintigraphy or MR. CT typically demonstrates unilateral or bilateral fracture lines in the sacral alae parallel to the SI joints. With healing the fracture lines may become sclerotic. CT can exclude destructive lesions such as malignancy and osteomyelitis, by demonstrating the trabeculae to be intact, apart from disruption at the fracture site. If the diagnosis is not certain, or if there is concern regarding healing, follow-up CT scanning after several months is useful.
Differential Diagnosis List
Final Diagnosis
Sacral Insufficiency Fractures
Liscense
Figures
Plain radiograph of Sacrum

T1-weighted axial MR image through sacrum

Gadolinium enhanced axial MR image through sacrum

Isotope bone scan, posterior view
CT scan through sacrum

Medical Imaging Analysis Report
I. Radiological Findings
1. X-ray: Pronounced osteopenia is observed in the lumbosacral region, with no significant abnormalities in the local soft tissue. However, relying solely on plain radiographs makes it difficult to accurately identify potential small fracture lines.
2. MRI: In the bilateral sacral ala (lateral mass of the sacrum), T1-hypointensity and T2/STIR hyperintensity suggest local bone marrow edema. Some sequences show a suspicious linear abnormal signal indicating a possible fracture line, although not very clear. No obvious soft tissue mass or abscess is noted.
3. Bone Scan (SPECT/Planar Imaging): Marked radioactive uptake on both sides of the sacrum is observed, and some patients may present a “butterfly” or incomplete “H-shaped” pattern of uptake. In this case, increased uptake in both sacral ala can be seen, forming a slightly “H-shaped” change.
4. CT: Subtle low-density fracture lines are observed in both sacral ala, oriented parallel to the sacroiliac joints. No obvious bone destruction or soft tissue mass is found. The bone structure remains relatively intact with interruption only at the fracture lines, consistent with suspected fractures. No erosive or destructive changes are seen in the local bone.
II. Potential Diagnoses
- Sacral Insufficiency Fracture (Stress/Osteoporotic Fracture):
Often seen in elderly females, frequently without a clear history of trauma, and commonly associated with osteoporosis. Radiologically, there may be edema-like T2 hyperintensity in the sacral ala, an “H-shaped” or butterfly-shaped uptake on bone scan, and a linear fracture line on CT. These findings match the current case. - Sacral Metastasis:
In patients with a history of malignancy, metastases should be considered. However, in this case, CT shows no obvious bone destruction or soft tissue mass, and the bone trabecular structure remains intact. MRI also shows no significant neoplastic lesions, making metastasis less likely. - Sacral Osteomyelitis (Infection):
Can present with bone marrow edema or abnormal signals, often accompanied by elevated inflammatory markers, severe pain, and soft tissue or paravertebral abscess. CT typically reveals bone destruction or sclerosis in the affected area. In this case, no such signs are seen, and there is no relevant infection history, making osteomyelitis less likely.
III. Final Diagnosis
Considering the patient’s age, gender (commonly elderly females), clinical presentation (pain aggravated by activity, no clear trauma history), radiological features (fracture lines in the sacral ala, edema signals, and an “H-shaped” radioactive uptake pattern), and excluding other destructive lesions, the most likely diagnosis is sacral insufficiency fracture (senile or osteoporotic sacral fracture).
IV. Treatment Plan and Rehabilitation
1. Conservative Treatment:
· Bed Rest and Pelvic Protection: Short-term bed rest or protected activity using a brace can be employed in the early stage to reduce sacral load and facilitate fracture healing.
· Pain Relief and Supportive Measures: Pain can be managed with analgesics (e.g., NSAIDs) or with physical support devices (hot compresses, physical therapy) to alleviate symptoms.
· Anti-osteoporosis Therapy: Oral or injectable bisphosphonates, calcium, vitamin D, and bone formation agents may be considered to accelerate fracture healing and prevent recurrent fractures.
2. Interventional or Surgical Treatment:
· For patients with severe symptoms, unstable fractures, or persistent pain, percutaneous sacroplasty or other internal fixation procedures may be considered. However, these are not typically first-line options.
· Surgical decision-making should involve specialist evaluation, considering overall health status, degree of osteoporosis, and fracture stability.
3. Rehabilitation and Exercise Prescription:
· FITT-VP Principles:
- Frequency: Begin with 3 sessions per week; once pain improves, increase to 4–5 times per week.
- Intensity: Start with low-intensity activities, such as simple core stabilization training (e.g., supine abdominal contractions), avoiding heavy weight-bearing or vigorous motion.
- Time: Begin with 10–15 minutes per session, gradually increasing to 30 minutes according to patient tolerance.
- Type: Include basic stretching, non-weight-bearing lower-limb exercises (sit-down pedaling, supine leg raises), and core training to strengthen the lumbar and dorsal musculature.
- Progression: As pain subsides and fracture healing progresses, gradually increase weight-bearing activities like standing or walking. Gentle resistance band training in a seated position can help strengthen muscles around the hip joint.
- Volume and Progress: Regular evaluations should guide incremental increases in exercise volume and variety if no significant pain or discomfort occurs.
· Precautions:
- Avoid high-impact or large-amplitude twisting of the waist before complete fracture healing.
- For elderly patients with osteoporosis or comorbidities (e.g., cardiopulmonary insufficiency), closely monitor heart rate, blood pressure, and respiratory status; watch for pain or discomfort during exercise.
- If severe pain, mobility limitation, or other abnormal symptoms arise, seek medical evaluation promptly.
Disclaimer
This report is a reference analysis based on the currently provided imaging data and clinical information; it does not replace an in-person consultation or the opinion of a qualified medical professional. If there are any questions or if symptoms worsen, please seek timely medical attention and follow the recommendations of a professional healthcare team.
Human Doctor Final Diagnosis
Sacral Insufficiency Fractures