Bilateral Osgood-Schlatter disease sequel


Clinical History
A 55-year-old female paatient was suffering from low back pain and bilateral knee and feet pain for four years.
Imaging Findings
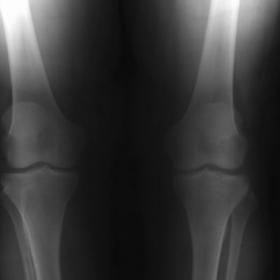
Our patient presented with suspected lumbar disc hernia. She was suffering from low back pain and bilateral knee and feet pain for four years. She said that she had bilateral knee pain, tenderness and swelling for one year when she was 10 years old, which limited itself. Lateral plain radiographs revealed an ossicle in bilateral distal patellar tendons (Fig. 1). Computed tomography showed bilateral fragments separated from tibial tuberosities, and the fragmented segments’ margins were sclerotic on both sides (Fig. 2).
Discussion
Osgood-Schlatter`s Disease (OSD) refers to partial avulsion of the tibia tuberosity, with no involvement of the tibial physis. OSD typically develops in girls between the ages of 8 and 13 and in boys between 10 and 15 years of age at the beginning of their growth spurt. This disease is more frequent in boys, and it may represent an overuse disease. It causes knee pain in children and teens which can be mild to severe. The condition usually goes away on its own over time but it may take months or years. The repetitive stress on tuberosity may cause partial avulsion. Radiographs will not be helpful if injury occurs during the preossification phase. Once an ossification center develops, radiographs will reveal radiodense fragments separated from tibial tuberosity. During periods of rapid growth, stress from contraction of the quadriceps is transmitted through the patellar tendon onto a small portion of the partially developed tibial tuberosity. This may result in a partial avulsion fracture through the ossification center. Approximately 25% of patients have bilateral lesions and their frequency of occurance is not known. Their etiology is unclear, but their condition is clearly exacerbated by exercise. Risk factors: Age between 11–18 years, male sex, rapid skeletal growth, repetitive jumping sports. Reported complications of Osgood-Schlatter's disease include fracture nonunion of the bone fragment, patellar subluxation, chondromalacia patellae and avulsion of the patellar tendon.
Differential Diagnosis List
Final Diagnosis
Bilateral Osgood-Schlatter disease sequel.
Liscense
Figures
X-ray



CT



1. Radiological Findings
Based on the provided X-ray (including anteroposterior and lateral views of both knees) and CT images, the main findings are as follows:
- The knee joint surfaces appear generally normal; there is no obvious severe narrowing of the joint spaces, but mild osteophyte changes (degenerative osteophytes) are observed in some areas.
- The tibial tuberosity region shows varying degrees of sclerosis or proliferative changes, possibly indicating chronic overuse changes or sequelae of previous tibial tubercle injury.
- The patella is generally normal in position and morphology, with no significant widening or narrowing of the medial or lateral meniscal spaces.
- CT images show that the patellar tendon and other joint soft tissues are within the normal range of density. At the tibial tuberosity, localized bone proliferation or sclerotic appearance suggests possible chronic irritation or old injury at the site of soft tissue attachment.
2. Possible Diagnoses
Taking the patient’s age, medical history (4 years of bilateral knee and foot pain), and radiological findings into consideration, the following diagnoses can be considered:
- Chronic inflammation of the tibial tuberosity or residual changes from Osgood-Schlatter disease
Although Osgood-Schlatter disease is more common in adolescents, it may leave ossifications or calcifications in adults, leading to chronic irritation and recurrent anterior knee pain. - Patellar tendon enthesopathy (patellar tendon insertion inflammation / “jumper’s knee”)
Chronic repetitive stress at the patellar tendon insertion on the tibial tuberosity can cause calcification or proliferation, resulting in similar symptoms. - Early osteoarthritis (OA) of the knee joint
The patient, aged 55, has had knee and foot pain for 4 years. Mild osteophytes seen on imaging might be related to early degenerative changes in the knee joint.
3. Final Diagnosis
Combining the patient’s age, duration of symptoms, and possible tibial tuberosity changes or evidence of old injury on imaging, the most likely diagnosis is:
“Chronic tibial tuberosity pathology (possibly residual adult Osgood-Schlatter disease with mild degenerative changes in the knee joint).”
The patient’s presentation could be due to incomplete resolution of Osgood-Schlatter disease during the growth period, leaving behind ossification or chronic inflammation at the tibial tuberosity. Additionally, mild to moderate degenerative changes associated with this age group may exacerbate symptoms. If further clarification is needed, an MRI of the knee joint can help rule out other soft tissue or meniscal pathology.
4. Treatment Plan and Rehabilitation
4.1 Conservative Treatment and Medication Management
- Anti-inflammatory and analgesic medications: Non-steroidal anti-inflammatory drugs (NSAIDs) may be used short-term during acute pain episodes or when pain is significant, to reduce inflammation and discomfort.
- Physical therapy: Modalities such as heat therapy, ultrasound therapy, and low-frequency electrical therapy can improve local blood circulation and alleviate inflammation.
- Orthotic supports: For significant discomfort around the tibial tuberosity, consider using knee braces or straps to reduce local stress.
4.2 Exercise Prescription (FITT-VP Principle)
Considering the patient’s age and prolonged symptoms, the exercise prescription should be gradual and individualized to reduce stress on the tibial tuberosity and knee joint:
- Frequency: 3–5 times per week.
- Intensity: Start with low-intensity activities, such as walking at an easy pace or using a low-resistance stationary bike. If available, consider aquatic rehabilitation exercises.
- Time: 20–30 minutes per session; initially, sessions can be divided into shorter segments (e.g., 10-minute sessions repeated 2–3 times).
- Type: Focus on low-impact aerobic exercises such as flat-ground walking, elliptical training, cycling, or water-based exercises. Avoid high-load movements like deep squats or jumping.
- Progression: Once pain subsides, gradually increase the duration of exercise or slightly increase resistance, avoiding sudden excessive increases in intensity or load.
Additional recommended exercises include:
- Quadriceps strengthening: For example, straight leg raises (lying supine, contract the quadriceps while raising the leg to around 30°–45°) or isometric contractions, performed slowly and gently to avoid aggravating tibial tuberosity discomfort.
- Partial squat exercises: Perform only when pain is mild or after pain has improved. Use support from a wall or handrail and limit squats to about 30°–45° of knee flexion to enhance muscle strength while minimizing stress on the tibial tuberosity.
- Hamstring and calf flexibility training: For instance, prone leg lifts and wall stretches for the gastrocnemius to improve overall flexibility and reduce anterior knee tension.
Disclaimer:
This report is a reference medical analysis based on the currently available imaging and medical history. It does not replace face-to-face consultations or professional medical advice. Should further concerns arise or symptoms worsen, please seek prompt evaluation at a qualified medical facility.
Human Doctor Final Diagnosis
Bilateral Osgood-Schlatter disease sequel.