Male with painless enlarged knee



Clinical History
A 66-year-old male with a history of knee infection with surgical debridement, presents with a long-standing painless enlarged left knee.
Imaging Findings
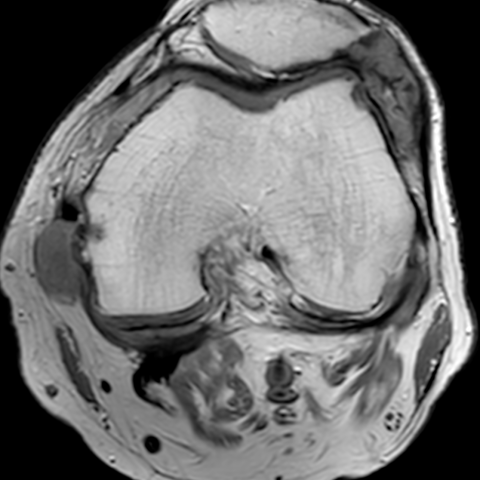
Axial proton density (PD) magnetic resonance imaging (MRI) of the left knee shows two heterogeneous intermediate-signal irregular oval-shaped lesions located in the lateral patellofemoral recess and adjacent to the medial collateral ligament (MCL), which erode the patellar and femoral surfaces (Figure 1a). Sagittal PD MRI of the same knee demonstrates the patellofemoral hyperintense lesion extending to the suprapatellar recess and showing no fat suppression (Figure 1b).
Axial computed tomography (CT) of the same patient shows the same lesions demonstrated by MRI, which are irregular and heterogeneously hyperdense, with better demonstration of cortical erosions (Figure 2a). Axial dual-energy CT (DECT) with color mapping shows uric acid deposits (orange) in the aforementioned lesions (Figure 2b). Three-dimensional DECT with color mapping shows uric acid depositions (blue) within knee joint and soft tissues (Figure 2c).
Discussion
Background and clinical perspective
Gout is a chronic disease of monosodium urate (MSU) crystal deposition and is one of the most common forms of inflammatory arthritis in adults, especially men [1].
Diagnosis of gout is traditionally based on characteristic clinical symptoms combined with elevated plasma urate levels and preferably joint/tophus aspiration with microscopical verification of MSU crystals [2]. However, aspiration is not always possible in routine clinical practice, and imaging techniques have gained an increasing role in the diagnosis of gout patients [2].
Imaging perspective
Various non-invasive imaging modalities such as radiography, sonography, conventional computed tomography (CT) and magnetic resonance imaging (MRI), have been used for the evaluation and diagnosis of gout [3]. Conventional CT can demonstrate erosions and hyperdense tophi with high sensitivity, though these findings remain of insufficient specificity for the diagnosis of gout. MRI can depict cortical erosions, marrow edema and gouty tophi, which may have variable signal characteristics depending on the amount of calcium present [4]. These imaging features, however, are not specific for gout, and often the diagnosis can only be inferred by correlating with disease distribution and other clinical features.
Dual-energy CT (DECT) offers the unique capability for the non-invasive detection of these crystals earlier in the course of the disease, as it can automatically color-code MSU depositions, based on predefined software settings. [3, 5]. It has been used to reveal the distribution and quantity of deposited MSU crystals in gout [4].
Outcome
Urate-lowering therapy (ULT) is a long-term management of gout to reduce serum urate levels, which can lead to dissolution of MSU crystals deposition, reduction or prevention of gout attacks, and joint damage [2, 6]. When left untreated, recurrent gout attacks and chronic gout inflammation can lead to severe structural damage to the painful bones, causing great harm to patients [1].
Take-home message / Teaching points
Gout is a chronic disease of MSU crystal deposition and is one of the most common forms of inflammatory arthritis in adults, especially men. Imaging findings play an important role in its diagnosis, especially when joint/tophus aspiration cannot be performed and as it provides specific information about the distribution and quantity of deposited crystals in soft tissues and joints.
All patient data have been completely anonymized throughout the entire manuscript and related files.
Differential Diagnosis List
Final Diagnosis
Knee gout
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures




Medical Analysis Report
Imaging Findings
The patient is a 66-year-old male presenting with long-term, painless swelling in the left knee. He has a history of knee joint infection and debridement surgery. Combining the provided MRI and CT images, the following features are observed:
- CT Plain Scan/Reconstruction: Multiple irregularly shaped high-density lesions can be seen on and deep within the left knee joint, with localized bone destruction and marginal sclerosis at the articular surface. Dual-Energy CT (DECT) reveals multiple high-density nodules with specific color coding, suggesting possible monosodium urate (MSU) crystal deposition.
- MRI Examination: Nodular or patchy lesions of low to intermediate signal intensity are observed within the soft tissue and around the joint capsule and synovium. On T1- and T2-weighted images, signals are heterogeneous. Some joint effusion is noted, along with abnormal synovial thickening. The articular cartilage surface is irregular, and there may be mild bone erosion in certain areas.
- Overall Presentation: Marked thickening of the soft tissues around the knee joint, with multiple nodular lesions and focal bone erosion. These imaging characteristics align with gouty arthritis (tophi) deposited in both the joint and surrounding soft tissues.
Potential Diagnoses
Based on the imaging findings and the patient’s history, the following diagnoses or differential diagnoses are considered:
- Gout (Tophus Formation): Deposition of monosodium urate crystals is the pathological basis of gout. Dual-Energy CT has high sensitivity and characteristic color coding for MSU crystals. Gout commonly occurs in middle-aged to elderly males, and can lead to destructive arthritis.
- Chronic Pyogenic Arthritis/Prosthesis-Related Infection: Given the patient’s history of infection and debridement, chronic inflammation or residual bacteria could cause ongoing joint destruction. However, it typically presents with recurrent pain or redness/swelling, and imaging often shows destructive changes and effusion.
- Rheumatoid Arthritis (RA): A common inflammatory joint disease that can cause erosive changes and soft tissue swelling around joints, usually in a symmetrical pattern, often accompanied by prominent clinical symptoms such as morning stiffness and pain.
Final Diagnosis
Considering the patient’s sex, age, long-standing painless knee swelling, past examination results (such as serum uric acid levels), and the characteristic crystal deposition identified by Dual-Energy CT, the most likely diagnosis is Gouty Arthritis (with multiple tophi).
For further confirmation, joint aspiration and microscopic crystal analysis (showing needle-shaped, negatively birefringent crystals) or monitoring of serum uric acid levels may be performed.
Treatment and Rehabilitation Plan
For gouty arthritis, the main treatment and rehabilitation strategies include:
- Pharmacological Treatment
- Uric acid-lowering agents (e.g., allopurinol, febuxostat) for long-term control of serum uric acid levels, reducing tophus formation and joint damage.
- During acute attacks, non-steroidal anti-inflammatory drugs (NSAIDs), colchicine, or short-term corticosteroids can be used to control inflammation.
- Lifestyle Modifications
- Dietary management: Restrict high-purine foods and alcohol intake. Increase fluid intake to promote uric acid excretion.
- Weight control: Obesity is associated with a higher risk of gout. Regular exercise and a healthy diet are recommended.
- Surgical Interventions
- In cases of large tophi, severe joint deformity, or functional impairment, surgical removal of tophi or joint replacement may be considered. Adequate preoperative evaluation is necessary to rule out infection or other complications.
- Rehabilitation and Exercise Prescription
- Initial Phase (Early Recovery): Focus on range-of-motion exercises and low-intensity aerobic activities. These may include gentle joint movements within tolerated levels of pain, bending and extension exercises, and low-resistance walking in water or cycling on a stationary bike.
- Middle Phase (Soft Tissue Adaptation): Gradually increase exercise intensity and frequency. Introduce light resistance exercises (such as using resistance bands or body weight). Perform sessions 3-5 times per week, 20-30 minutes each, monitoring joint response to avoid excessive load.
- Later Phase (Strength and Endurance Building): Once inflammation is well controlled, moderately increase strength training and aerobic exercise duration. Gradually transition to moderate-intensity strength exercises, walking, or light jogging. Conduct 3-5 sessions per week, 30-45 minutes each.
- Continuous Monitoring (FITT-VP): Throughout rehabilitation, dynamically adjust Frequency, Intensity, Time, Type, Progression, and Volume of exercise based on the patient’s joint response and overall condition.
- Safety Precautions: If the patient experiences joint swelling, pain, or unusual discomfort, reduce activity or seek medical advice promptly.
Disclaimer: This analysis report is for reference only and does not replace in-person consultation or professional medical advice. If you have any questions or changes in condition, please consult a medical professional promptly.
Human Doctor Final Diagnosis
Knee gout