Extraskeletal mesenchymal chondrosarcoma



Clinical History
A 40 year old man with a palpable mass on the right thigh, with a progressive increase in size for the last five months.
Imaging Findings
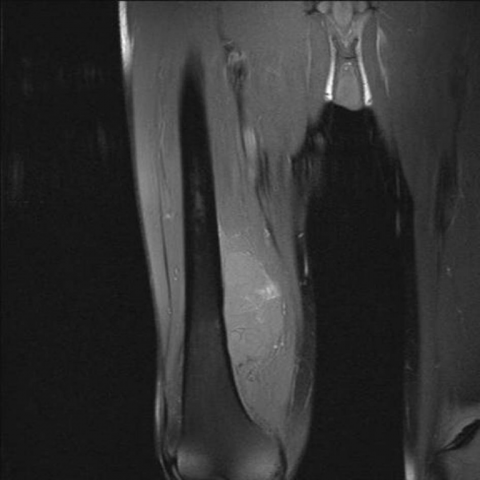
40 year old man referred to our institution for a painless palpable mass on the anteromedial aspect of his right thigh with no surrounding erythematous reaction. Doppler ultrasound examination was performed, demonstrating an oval shaped lesion with heterogeneous echostructure and increased vascularity. Magnetic Resonance Imaging (MRI) study depicted a soft tissue mass involving the anterior, medial and posterior compartments of the right thigh, with infiltration of the vastus (intermedius and medial), adductor brevis, biceps femoris, semi membranous and semitendinous muscles. Invasion of the femoral cortical bone in the postero-medial aspect of the distal diaphysis with associated invasion of the medullary cavity was also seen. The superficial femoral artery and vein as well as the sciatic nerve were surrounded by the tumoral mass. The mass demonstrated high signal intensity on T2-weighted images (fig.1), and areas of high signal intensity on fat suppressed T1-weighted images, consistent with hemorrhagic foci (fig 2). On Gadolinium enhanced images, the mass had a heterogeneous enhancement (fig.3). The findings were compatible with an aggressive soft tissue mass. Hystologic analysis demonstrated areas of well defined cartilage, associated with areas of neoplasic proliferation of the mesenchyma, formed by packs of small cells with oval hyperchromatic nuclei clustered together, along with vascular clefts and areas of necrosis (fig.4).
Discussion
Extraskeletal mesenchymal chondrosarcoma (EMC) was first reported as a distinct entity by Lichtenstein and Bernstein in 1959. It was described as an uncommon, aggressive variant of chondrosarcoma with a strong tendency to metastasize to distant sites. This tumor commonly arises in bone but in approximately 30% of cases it arises in extraskeletal locations (1), such as the central nervous system, soft tissue and mediastinum (2). EMC has a bimodal age distribution; tumors in the head and neck occur primarily in the 3rd decade of life, whereas those in the thigh occur most frequently in the 5th decade of life (3, 4). Clinical symptoms are non-specific, with the most common finding being a slowly enlarging painless soft-tissue mass (5). The lesion has an aggressive clinical course and metastases are frequent, usually to the lungs and lymph nodes (2, 4, 5). EMC is composed predominantly of sheets of undifferentiated mesenchymal cells with differentiated cartilaginous component usually comprising only a small percentage of the lesion (2, 3). The imaging evaluation of a suspected EMC begins with conventional radiographs, that may show calcifications, which can suggest the diagnosis, and can also reveal osseous involvement (6). Some reports say that fifty percent to 100% of EMC demonstrate arc, ring, stippled and highly opaque calcifications at conventional radiography on Computed Tomography (CT) (3, 4). MRI is the preferred modality for evaluating EMC, demonstrating the configuration of the tumor and extent of the mass (3, 6). Despite the superiority of MRI in identifying, delineating and staging EMC, it remains limited in its ability to characterize it precisely, with most lesions demonstrating high signal intensity on T2 weighted images, isointensity to the muscle on T1 weighted images, and high heterogeneous enhancement after intravenous gadolinium injection (6), as can be seen in our patient.Likewise, some publications describe characteristic findings on the EMC related to the pattern and extension of the intratumoral mineralization, which can form two clearly delineated areas. This calcified areas show low signal intensity both on T1 and T2 weighted images, while the non calcified areas are isointense to muscle on T1-weighted images and of intermediate signal on T2-weighted images. EMC typically presents with a lower signal intensity on T2-weighted images in comparison to other types of chondrosarcoma due to its higher cellularity and to its smaller water content (2,5). After contrast administration EMC presents an intense and heterogeneous enhancement, due again to its high cellularity. Although in given cases we can diagnose EMC from the radiologic appearance, final diagnosis must be confirmed with the histological results in order to set up the adequate therapeutic course. Imaging provides valuable information of staging and also helps guide biopsy of the tumor to obtain representative samples.
Differential Diagnosis List
Final Diagnosis
EXTRASKELETAL MESENCHYMAL CHONDROSARCOMA
Liscense
Figures
Axial T2-weighted image

Coronal fat-suppressed T1-weighted image
Coronal fat-suppressed T1-weighted image after gadolinium administration

Histological sample of the soft tissue mass

Imaging Findings
The patient’s right thigh MRI shows a clearly visible soft tissue mass with an irregular shape. The tumor’s signal characteristics are as follows:
- T1 Weighted Image: The lesion appears approximately isointense compared to muscle, with some slightly lower or mixed-signal areas.
- T2 Weighted Image: The lesion appears predominantly hyperintense, but within it are areas of relatively low signal, suggesting possible calcification or fibrous components.
- Contrast-Enhanced Scan: The mass shows marked heterogeneous enhancement, indicating a rich blood supply and complex internal components.
MRI findings reveal that the lesion involves the soft tissue of the thigh. The borders are partially well-defined, while in some areas the delineation from surrounding tissues is less clear. No definite bony destruction is observed, but potential cortical erosion or intramedullary involvement should be carefully ruled out. There is no obvious compression or deformation of nearby vascular and nerve structures, though correlation with involvement of surrounding muscle groups is recommended.
Potential Diagnoses
-
Chondrosarcoma (especially extraskeletal chondrosarcoma/mesenchymal chondrosarcoma):
According to the literature, such tumors can present with cartilaginous signal characteristics (high T2 signal), often accompanied by calcifications or cartilaginous matrix, and show significant enhancement. The patient’s age (40 years) and the rapid enlargement over the past five months fit this possibility.
-
Liposarcoma or Other High-Grade Soft Tissue Sarcomas:
Some high-grade sarcomas can also exhibit cartilaginous or cartilage-like components, with a markedly high T2 signal and irregular morphology, sometimes mixed-signal. The fast growth rate requires differentiation from other entities.
-
Fibrosarcoma or Undifferentiated Pleomorphic Sarcoma:
Although T2 signal is often high, low-signal components may also appear. Histological and pathological evaluations are needed to distinguish these tumors.
Final Diagnosis
Combining the patient’s age, clinical presentation (a gradually enlarging soft tissue mass), MRI findings suggesting distinct cartilaginous matrix or calcification, and histopathological evidence supporting “Mesenchymal Chondrosarcoma (Extraskeletal Mesenchymal Chondrosarcoma, EMC)”, the most consistent diagnosis is Extraskeletal/Mesenchymal Chondrosarcoma.
If imaging alone cannot completely rule out other soft tissue sarcomas, additional evaluations with pathology and immunohistochemistry are necessary. If pathological confirmation has already been obtained, the diagnosis is more definitive.
Treatment Plan and Rehabilitation
Treatment Strategy
- Surgical Treatment: A radical resection is the primary treatment option, aiming to achieve clear surgical margins. Based on intraoperative and postoperative pathology, chemotherapy and/or radiotherapy may be required.
- Adjuvant Therapy: Given the high malignancy of mesenchymal chondrosarcoma, comprehensive treatment—usually including chemotherapy and radiotherapy—often follows a pathological diagnosis to reduce recurrence and the risk of distant metastases.
Rehabilitation/Exercise Prescription
Rehabilitation should follow a gradual, individualized approach. Below is a sample guideline:
- Early Postoperative Phase (Tissue Repair Stage):
- The main goals are to protect the affected limb and prevent thrombosis and circulation issues. Low-intensity exercises such as ankle pumps and straight leg raises (if not impacting the surgical site) can be performed.
- Frequency: 2-3 times per day; Duration: 10-15 minutes each time, with slow movements.
- Intermediate Phase (Strength and Joint Mobility Recovery):
- Under the guidance of a physician or rehabilitation therapist, strengthen the lower limbs, restore joint mobility, and train core muscles (e.g., knee flexion and extension exercises, hip exercises in seated or supine positions).
- Frequency: 3-4 times per week; Intensity: maintain heart rate at 50-60% of maximum; Duration: around 30 minutes per session.
- Late Phase (Functional Reconstruction and Return to Daily Life):
- Gradually increase exercise intensity, including posture and gait training, light resistance exercises (e.g., low-weight resistance training), and low-impact aerobic activities (such as stationary cycling or swimming).
- Frequency: 3-5 times per week; Intensity can be increased to 60-70% of maximum heart rate; Duration: 30-45 minutes.
Throughout the rehabilitation process, monitor for pain, swelling of the affected limb, and overall systemic reactions. If any abnormal symptoms occur, seek medical attention or adjust the rehabilitation plan promptly.
Note: Because tumor surgery and comprehensive treatments can cause bodily damage, patients may have weaker bones and reduced cardiopulmonary reserve. Exercise intensity should be adjusted carefully, and precautions should be taken to avoid falls or re-injury.
Disclaimer
This report is based on existing clinical and imaging data and is provided for reference only. It is not a substitute for an in-person consultation or a treatment plan designed by a professional doctor (especially in orthopedics and oncology). If you have concerns or if symptoms worsen, please visit a hospital or seek further evaluation and management from a specialist.
Human Doctor Final Diagnosis
EXTRASKELETAL MESENCHYMAL CHONDROSARCOMA