Multiple Myeloma with an Unusual Distribution of Bony Involvement. Report of a Case


Clinical History
Fatigue, malaise and right heel pain
Imaging Findings
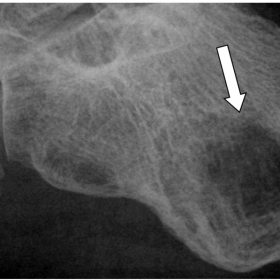
44-year-old male with a one month history of fatigue, malaise and heel pain. The following haemaological abnormalities were identified at presentation: Low Haemoglobin of 7g/dl. Raised ESR of 150. Total globulins elevated at 80. IgA of 79. Serum electrophoresis revealed a localised band in the alpha region thus confirming IgA myeloma. Skeletal survey unusually showed no bony abnormality. Plain radiograph of the painful heel (Fig 1) demonstrated a well circumscribed radiolucent lesion within the calcaneum measuring 2cm x 2cm in diameter. This radiological appearance looked suspicious for that of a myelomatous deposit. Percutaneous biopsy of this lesion confirmed the presence of abundant neoplastic plasma cells within the calcaneum. Progression of bone pain in both feet revealed multiple punched out lytic lesions in a predominantly periarticular distribution within the bones of the tarsus and the metatarsals (Figs 2 and 3). This is a characteristic radiological manifestation of the osteolysis associated with multiple myeloma. Radiograph of the forearm (Fig 4) also demonstrated another prominent feature of multiple myeloma – that of endosteal scalloping. This is due to erosion of the inner border of the cortex of the proximal radius caused by myelomatous deposits. A solitary lytic lesion was also seen in the proximal right tibia (Fig 5).Plain radiographs of the wrist (Fig 6) also showed involvement of these areas by periarticular diffuse myelomatosis. Disease in the axial skeleton was never demonstrated.
Discussion
Multiple myeloma or plasma cell myeloma is the most common primary malignant process in adults, representing around 1% of all malignancies and approximately 10% of the total number of haematologic malignancies[1]. 97% of cases occur in adults over the age of 40 with a slight male preponderance[2]. It is one of a spectrum of conditions arising from dysfunction of the plasma cell. A series of genetic changes leads to formation of a clonal neoplasm of plasma cells of B lymphocyte origin. Uncontrolled plasma cell proliferation occurs without any stimulus by an antigen. This results in excessive quantities of globulins or their subunits being produced. In addition, changes in the microenvironment of the bone marrow enhances tumour growth and overproduction of monoclonal immunoglobulins and prevents the immune system from controlling disease progression[4]. In the vast majority of cases plasma cell infiltration first appears in the axial skeleton and therefore the first radiological manifestations of multiple myeloma become apparent in the vertebrae, ribs, skull and pelvis[3]. The rapidly expanding population of malignant plasma cells compromises the integrity of bones by physically replacing and eroding the native architecture of the bony trabeculae. The malignant clones also inhibit bone formation and stimulate bone resorption by invading the marrow, adhering to marrow stromal cells and stimulating production of osteoclast-activating factors[5]. Clinically, the most common presenting symptom is that of bone pain. Fatigue and lethargy are also frequently encountered and result from the underlying malignancy as well as anaemia. Patients may also experience increased incidence of infection due to suppression of normal immunoglobulin synthesis. As well as causing symptoms resulting from bone pain and destruction up to 30% of patients suffer from the effects of elevated serum calcium (more often in advanced disease). The most characteristic and frequently seen pattern of bone destruction in multiple myeloma is the presence of either solitary or multiple areas of osteolysis and is seen in over 90% of patients. In the majority of patients with the common osteolytic form of multiple myeloma the axial skeleton is the first site of disease involvement. Eventual spread to the extremities may occur but usually only after disease has been well established in sites such as vertebrae and ribs. Rarely, multiple myeloma with exclusive involvement of the appendicular skeleton has been described but in almost all of these cases it has been in association with concurrent disease of central haemopoeitic sites such as myelofibrosis[3]. This patient has no such synchronous disease process. To the best of our knowledge, a distribution of multiple myeloma such as this is indeed unusual and represents yet another facet of the many manifestations of this widely prevalent condition.
Differential Diagnosis List
Final Diagnosis
Mutiple Myeloma with sparing of the axial skeleton.
Liscense
Figures
Fig 1. Calcaneum

Fig 2. Tarsus

Fig 4. Forearm

Fig 5. Proximal Tibia.

Fig 3. Metatarsals

Fig 6. Wrist.

Medical Imaging Analysis Report
I. Radiological Findings
Based on the provided X-ray images of the foot, tibia, and fibula, the following observations are noted:
- Multiple lytic lesions with relatively clear boundaries (indicated by arrows) are visible in the bone, appearing round or nearly round.
- Significant cortical thinning is observed in the calcaneus, metatarsals, and parts of the tibia, along with reticular or honeycomb-like radiolucent areas.
- No obvious soft tissue masses are identified, but the extent of bone destruction is considerable, indicating decreased bone strength.
- No obvious fracture lines are seen; however, if the lesions progress further, there is an increased risk of fracture.
II. Potential Diagnoses
Considering the patient’s age (44 years old), symptoms (fatigue, general malaise, heel and lower extremity pain), and the radiological presentation (multiple lytic lesions), the following differential diagnoses are suggestive:
- Multiple Myeloma: A common primary malignant bone marrow tumor in adults, accounting for around 10% of hematologic cancers. Typical presentations include multiple lytic bone lesions, bone pain, and fatigue. The patient’s age, clinical symptoms, and imaging findings are consistent with these hallmarks.
- Bone Lymphoma or Metastatic Bone Tumors: Bone lymphoma can present as lytic bone lesions, though often it appears as a single destructive lesion; metastatic bone lesions may also present with lytic changes, necessitating further investigations to identify any primary site.
- Rare Bone Infection (Chronic Osteomyelitis): Can show lytic areas, but often accompanied by soft tissue inflammation, local swelling, and indicative signs of infection. Local symptoms are usually more pronounced.
III. Final Diagnosis
In summary, taking into account the patient’s age, clinical manifestations (fatigue, bone pain), laboratory indicators (including immunoglobulin levels, blood count changes, elevated protein levels, anemia, renal function impairment, etc.), and the multiple lytic lesions observed on X-ray, the most likely diagnosis is:
Multiple Myeloma (also known as plasmacytoma)
If there is still uncertainty, further testing such as serum protein electrophoresis, bone marrow biopsy, or a bone scan/whole-body PET-CT can be performed to confirm the final diagnosis.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Pharmacotherapy: Commonly involves chemotherapy (e.g., lenalidomide, proteasome inhibitors) in combination with corticosteroids; autologous hematopoietic stem cell transplantation may be considered when appropriate.
- Bone Protection: Based on fracture risk and the degree of bone destruction, bisphosphonates (such as zoledronic acid) or other bone-protective agents are routinely used to slow the progression of bone damage.
- Radiotherapy: For severe localized pain or high-risk lesions (likely to fracture), focused radiation therapy can help control pain and stabilize the lesions.
- Surgical Treatment: In cases of severe bone structure destruction or high risk of pathological fracture, surgical fixation and reconstruction may be considered.
2. Rehabilitation and Exercise Prescription
Because multiple myeloma leads to fragile bones, the following principles should be observed when formulating an exercise prescription:
- Gradual Progression: Begin with low-intensity, short-duration daily activities (e.g., walking or gentle indoor activities) and gradually increase the exercise amount.
- Individualization: Tailor the exercise regimen based on the patient’s bone strength, cardiorespiratory fitness, and fatigue levels. Consult specialists or physical therapists if needed.
- Type of Exercise: Emphasize mild aerobic exercise (e.g., walking on flat surfaces, stationary cycling) and light resistance training, avoiding high-impact or heavily weighted exercises.
- Frequency: Exercise 3–5 times per week, ensuring no excessive fatigue or worsening of pain.
- Intensity: Begin at a level that feels “somewhat hard” subjectively; patients with fragile bones must avoid vigorous or jumping movements.
- Time: Each session should initially last 20–30 minutes, gradually extending to 45 minutes or more, while closely monitoring fatigue.
- Type: Safe options include walking, seated cycling, and stretching exercises.
- Progression: As disease control improves and physical condition strengthens, gradually increase exercise duration or add light resistance, ensuring no significant bone pain or complications occur.
During this period, prevent falls or external impacts. If severe pain or discomfort arises, seek medical advice or contact the rehabilitation team promptly.
Disclaimer
This report is offered as a reference based on the available imaging and clinical information and does not replace in-person consultations or professional medical advice. If you have any doubts or if symptoms worsen, please seek medical attention promptly for a personalized and professional treatment plan.
Human Doctor Final Diagnosis
Mutiple Myeloma with sparing of the axial skeleton.