Partial Rupture of Triceps Tendon



Clinical History
Triceps tendon ruptures are rare. We report a case of a partially ruptured triceps tendon in a fit and healthy bodybuilder.
Imaging Findings
A 44-year old man presented with pain in his right upper arm. He was a bodybuilder and, following a trivial fall onto his flexed right elbow, had subsequently tried to return to his gym activities during which he felt a sudden severe sharp pain in the right posterior upper arm on extending his elbow to resistance. There was no significant past medical history and denied any drug use. Clinically, he had swelling and tenderness proximal to the olecranon process with a boggy swelling over the distal triceps. He had weakness in extending his elbow but was nevertheless able to actively extend it. There were no sensory neurological symptoms or signs.
Plain radiography of his elbow revealed an olecranon traction spur as well as bony avulsion fragments proximal to the distal olecranon.
An ultrasound scan was subsequently performed. This showed partial rupture of the distal triceps tendon, involving the superficial fibres. The superficial fibres were retracted and lay approximately 5cm above the olecranon process. A small haematoma was noted at the site of rupture. The deep fibres were intact. Fragments of bone were also noted at this site, consistent with the plain radiograph findings of an avulsed fragment of the olecranon. Ultrasound of his left elbow, performed for the purpose of comparison, was within normal limits.
The patient was treated conservatively with the elbow held in partial flexion. He gained a full range of motion and is currently undergoing strengthening exercises, which he is expected to fully regain.
Discussion
Triceps tendon rupture is an uncommon injury. The tear usually occurs at the tendon-osseous junction and is usually accompanied by avulsion fractures of the olecranon process [1]. The majority of ruptures occur following a fall onto the outstretched hand or following direct impact to the arm [1]. However, the injury is also recognised in patients whilst weight lifting [2]. Partial rupture of the tendon is even more rare. Clinical diagnosis is usually obvious but the findings may occasionally be subtle or difficult to assess because of swelling and pain. In this case, the fact that the patient could extend his elbow, although weakly, suggested an incomplete rupture and highlights the need for imaging. MRI provides an excellent overall view of the elbow extensor mechanism and the extent of a tear and muscle retraction [3]. However, ultrasound, together with clinical examination, will often provide the adequate information necessary in order to formulate a management plan, as in this case. Furthermore, the dynamicity of ultrasound gives it obvious advantages over other imaging modalities. Ultrasound should therefore always be considered as the first radiological investigation in suspected triceps ruptures.
Most surgeons will repair complete ruptures surgically. There is, however, no consensus to support either operative or conservative management in partial ruptures, but these are successfully reported in the literature [4]. In our case, conservative management was chosen and proved successful.
Differential Diagnosis List
Final Diagnosis
Partial rupture of triceps tendon
Liscense
Figures
X-ray

Ultrasound of normal left elbow
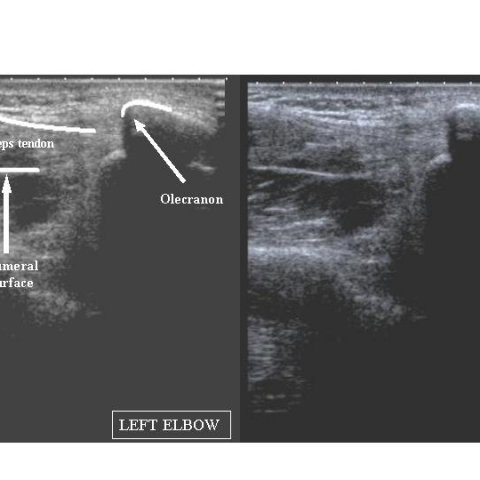
Ultrasound of partially ruptured right triceps tendon

Imaging Findings
The patient is a 44-year-old male bodybuilding enthusiast, presenting clinically with reduced elbow extension strength but still able to partially extend the elbow. Based on the X-ray and ultrasound images, the main findings are as follows:
- X-ray: A small free bone fragment or avulsion fracture fragment is visible at the ulna’s olecranon, and a traction spur (“Olecranon traction spur”) is also observed at the olecranon site.
- Ultrasound: Shows partial disruption of fiber continuity at the triceps tendon insertion on the olecranon, with a small amount of hematoma or effusion; deeper fibers remain intact. A corresponding hyperechoic or irregular echo is seen for the avulsed bone fragment.
Overall, the imaging findings suggest a partial tear of the triceps tendon, and the avulsed bone fragment along with local hematoma further indicates injury at the tendon insertion.
Possible Diagnoses
- Partial Tear of the Triceps Tendon: Imaging and clinical exams both indicate localized fiber discontinuity, but partial active elbow extension is still possible, pointing to an incomplete (partial) tear.
- Complete Tear of the Triceps Tendon: In a complete tear, the patient typically cannot actively extend the elbow. However, in a few cases, compensation by other muscle groups may create the appearance of retained function, so imaging is necessary to rule it out.
- Olecranon Avulsion Fracture or Local Tendon Insertion Injury: An avulsed bone fragment is visible on the X-ray, so a fracture should be considered. However, based on clinical function and ultrasound findings, a partial triceps tendon tear with an avulsed bone fragment is more consistent with this case.
In summary, local avulsion fractures should be distinguished from tendon injuries, but this case is more suggestive of a partial tear of the triceps tendon with an associated avulsed bone fragment.
Final Diagnosis
Based on the patient’s age, history of bodybuilding, clinical symptoms (weakness in extending the elbow but still able to partially extend), and the imaging evidence, the most likely diagnosis is:
Partial Tear of the Triceps Tendon (with Avulsed Bone Fragment)
No further histological biopsy is currently required. Typically, high-resolution ultrasound or MRI is used to determine the extent of the tear and to decide whether surgical intervention is needed.
Treatment Plan and Rehabilitation Protocol
For a partial tear of the triceps tendon, conservative management is generally considered first. In cases of complete tear or severe instability, surgical repair is often required.
- Conservative Treatment:
- In the early stage, a brace or cast can be applied to maintain the elbow in slight flexion, reducing secondary injury.
- Use non-steroidal anti-inflammatory drugs (NSAIDs) to relieve local pain and inflammation, along with local physiotherapy (e.g., cold therapy, ultrasound therapy).
- Schedule regular follow-up ultrasound or imaging to monitor the healing of the tear.
- Surgical Treatment:
- If imaging reveals a large-scale tear, significant displacement, or severe functional impairment, surgical repair or reconstruction may be performed.
- For larger avulsed bone fragments compromising joint stability, surgical internal fixation should be considered.
Rehabilitation/Exercise Prescription (FITT-VP principle):
- Early Phase (0–2 weeks post-injury):
- Frequency: 1–2 sessions of mild activity per day.
- Intensity: Should not cause significant pain; avoid weight-bearing or resistance training.
- Time: 5–10 minutes per session, mainly focusing on passive joint motion and gentle stretching.
- Type: Mild joint movement exercises (such as gradual flexion and extension after immobilization is lifted) and light isometric muscle contractions.
- Progression: Adjust the range of motion and activity frequency weekly according to pain and swelling.
- Intermediate Phase (2–6 weeks post-injury):
- Frequency: 3–4 times per week.
- Intensity: Introduce low-load resistance exercises (e.g., resistance bands), gradually strengthening both isometric and isotonic exercises for the triceps.
- Time: 15–20 minutes per session, gradually increasing as tolerated.
- Type: Continue range-of-motion exercises combined with local muscle strengthening.
- Progression: Increase resistance and range of motion gradually, ensuring no onset of pain.
- Late Phase (after 6 weeks):
- Frequency: 3–5 times per week, gradually increasing to an acceptable daily or athletic level.
- Intensity: Gradually return to equipment-based training, but avoid excessive weights to prevent re-injury.
- Time: 20–30 minutes per session, combining aerobic and resistance exercises.
- Type: Comprehensive functional training, including proprioceptive (balance, coordination) and core strengthening exercises.
- Progression: As function recovers, slowly resume regular bodybuilding routines, carefully monitoring joint response.
Throughout the rehabilitation process, closely observe pain, swelling, and strength recovery. Adjust the rehabilitation plan if necessary to ensure safety and effectiveness.
Disclaimer: This report is intended for medical reference only and is not a substitute for a face-to-face diagnosis or professional medical advice. If you have any questions or changes in your condition, please consult a specialist or seek hospital care promptly.
Human Doctor Final Diagnosis
Partial rupture of triceps tendon