ALPSA lesion and Buford complex in an unstable shoulder



Clinical History
Recurrent anterior dislocation of left shoulder
Imaging Findings
32 year old professional guitarist who first dislocated his shoulder playing American football ten years back. Since then he has had at least seven complete anterior dislocations and innumerable partial events. The last episode occurred during sleep while he was putting his hand behind his head. After relocating the shoulder in the Accident and Emeregency department, the patient had an outpatient orthopaedic referral. On examination in the clinic, he had a normal shoulder contour and a functioning axillary nerve. He had full range of movements. Apprehension test and anterior relocation test were positive.
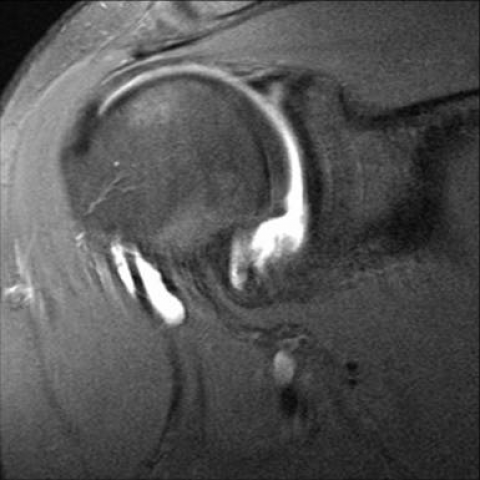
An MR arthrogram was performed which showed detachment of the anteroinferior glenoid labrum with intact scapular periosteum and a Hill Sach’s defect in postero superior humeral head. Other findings included a posterior labral tear, absent anterosuperior glenoid labrum along with thickened middle gleno humeral ligament. Arthroscopy confirmed the anterior labral detachment and a Bankart repair was performed.
Discussion
Anteroinferior instability is the most common type involving the glenohumeral joint, occurring in 95% of patients (1). Tears of the labroligamentous complex is a frequent association often with fractures of the bony glenoid and humeral head. MR arthrogaphy is now the investigation of choice and provides excellent depiction of the intra articular structures. In anterior labroligamentous periosteal sleeve avulsion (ALPSA lesion) the torn anteroinferior labrum is displaced inferomedially but remains attached to the scapula by an intact scapular periosteum. In our case this was associated with a congenitally absent anterosuperior labrum and a thickened middle glenohumeral ligament which together is referred to as the Buford complex.
Differential Diagnosis List
Final Diagnosis
ALPSA lesion, Hill Sachs defect, Buford complex.
Liscense
Figures
PD fat suppressed axial shoulder MR arthrogram.

PD fat suppressed axial shoulder MR arthrogram. ABER position.

PD fat suppressed coronal shoulder MR arthrogram.
PD fat suppressed sagittal oblique MR arthrogram

Medical Imaging Analysis Report
Patient Information: 32-year-old male with a history of repeated anterior dislocation of the left shoulder.
I. Imaging Findings
According to the provided MR arthrogram images of the shoulder joint:
- Anterior inferior glenoid rim: An anterior inferior labrum structure continuous with the supraglenoid labrum is displaced inferiorly, showing irregular shape and abnormal signal, suggesting a labral tear involving its attachment.
- The anterior inferior joint capsule and the labrum have not completely separated from the scapular periosteum, indicating intact relationship with the scapular periosteum (outer layer). However, the labrum has moved medially and inferiorly, consistent with an ALPSA (Anterior Labral Periosteal Sleeve Avulsion) lesion.
- There is congenital absence of the anterosuperior labrum and a significantly thickened middle glenohumeral ligament, consistent with a “Buford complex.”
- No obvious signs of tearing are seen in other structures of the shoulder joint (such as the supraspinatus tendon, infraspinatus tendon, or joint cartilage). The humeral head and glenoid bone signal are generally unremarkable, but there is mild cortical irregularity possibly due to bone contusion or repeated impaction.
II. Possible Diagnosis
Based on the imaging findings and the history of recurrent anterior shoulder dislocation, the following diagnoses can be considered:
- ALPSA (Anterior Labral Periosteal Sleeve Avulsion) lesion: Compared to a Bankart lesion, ALPSA involves an anterior inferior labrum that is avulsed but remains attached to the scapular periosteum, thereby shifting medially and inferiorly, which aligns with the imaging features of this case.
- Bankart lesion: If both the labrum and the periosteum are torn and detached, a typical Bankart lesion may form. In this case, the findings are more consistent with ALPSA. However, clinically, recurrent shoulder instability also requires ruling out Bankart lesions or Hill-Sachs lesions of the humeral head.
- Buford complex: Congenital absence of the anterosuperior labrum with a thickened middle glenohumeral ligament attaching to the joint cavity is a normal variant. It has a relatively low correlation with recurrent shoulder instability, but should be carefully identified during surgical evaluation and repair so it is not overly corrected.
III. Most Likely Final Diagnosis
Considering the history of recurrent anterior shoulder dislocation, MRI arthrogram findings of a medially and inferiorly displaced anterior inferior labrum that remains attached to the periosteum, as well as congenital anterosuperior labral absence with a thickened middle glenohumeral ligament, the most likely diagnosis is:
- ALPSA (Anterior Labral Periosteal Sleeve Avulsion) lesion combined with a Buford complex
This combination is relatively rare but matches the imaging features and congenital variant seen in this case.
IV. Treatment Plan and Rehabilitation
For ALPSA lesions and common causes of shoulder instability, the following treatment strategies may be considered based on the severity of the lesion and the patient’s functional needs:
- Conservative management: If the number of dislocations is low or symptoms are relatively mild, the patient can initially undergo shoulder immobilization and physical therapy. An abduction brace or protective shoulder support can be used to limit movement, combined with anti-inflammatory and pain-relieving medications to reduce pain and inflammation.
- Arthroscopic repair: For patients with significant symptoms, frequent dislocations, or severe labral tears, arthroscopic surgery to repair the anterior labrum and tighten the joint capsule and related ligamentous tissue may be considered. For Buford complexes, careful intraoperative differentiation of this normal variant is required to avoid excessive repair.
Rehabilitation and Exercise Prescription:
- Early phase (postoperative or immobilization period, 0–4 weeks): Focus on passive range of motion exercises to maintain joint mobility and prevent excessive stiffness from immobilization. Perform 1–2 sessions per day, each session lasting about 15 minutes, with very light intensity.
- Middle phase (4–8 weeks): Gradually progress to active range of motion and light resistance training, focusing on restoring muscle strength around the shoulder. Exercises with resistance bands for abduction and adduction can be introduced. Frequency: 3–4 times per week, 20–30 minutes per session, with light to moderate intensity.
- Late phase (8–12 weeks): Strengthen functional training, enhance shoulder stability and coordination through exercises such as planks and dumbbell or sandbag exercises for shoulder-muscle groups. Frequency: 3–5 times per week, over 30 minutes per session, with moderate intensity and a gradual increase in weight.
- Advanced phase (after 3 months): Gradually return to overhead throwing activities or any large range-of-motion movements required in daily life, according to the patient’s condition. For gym or sports activities, progression in intensity and load should be guided by a professional therapist or trainer.
- Note: Patients with chronic overuse or recurrent shoulder instability should maintain regular muscle strengthening exercises in daily life, especially for the rotator cuff and scapular stabilizers, to improve proprioception and shoulder stability.
Disclaimer: This report is based solely on available imaging and medical history for reference and cannot replace in-person consultation and professional medical advice. Specific treatment and rehabilitation plans should be formulated by an orthopedic or sports medicine specialist based on the patient’s clinical condition.
Human Doctor Final Diagnosis
ALPSA lesion, Hill Sachs defect, Buford complex.