Severe posterior knee injury



Clinical History
A 47-year-old construction worker fell in a street shaft and distorted his left knee. Knee MRI revealed a posterior cruciate ligament tear and an injury of the posterolateral complex. Primary therapy remained conservative.
Imaging Findings
A 47 year old construction worker fell in a street shaft and distorted his left knee. He presented with severe pain, a reduced mobility (extension - flexion 0 - 0- 90°) and a slight joint effusion. X-ray and multislice- CT excluded a fracture. Because of continuing pain and increasing joint effusion MRI of the knee was performed (Siemens Harmony 1.0 T, Knee coil, T1SE cor, Tirm cor, T2TSE tra, T2*medic sag 4 mm slices and T2TSE sag angled for the cruciate ligaments 3 mm slices).
Besides a rupture of the posterior cruciate ligament (Figure 1), a tear of the myotendinous junction of the popliteus muscle was diagnosed (Figure 2, 3) and an extensive edema of its muscle belly was visible (Figure 4, 5). The attachment to the lateral femoral sulcus was intact (Figure 6). Motoricity and sensibility of the leg were not impaired. A posterolateral instability was not stated by physical examination. Primary therapy remained conservative.
Discussion
The popliteus muscle is an important structure for posterolateral stabilization of the knee and arises from the lateral femoral condyle and attaches at the posterolateral margin of the proximal tibia. Its tendon attaches to the posterior horn of the lateral meniscus and the fibular head. Beside its function as a stabilizer the muscle is the initiator of internal rotation in a "non weight bearing state" [1].
Injuries of the posterolateral complex (consisting of popliteus, ligamentum arcuatum, lateral collateral ligament et al.) are less common than medial or anterolateral knee injuries and are usually combined with cruciate ligament ruptures. LaPrade et al. reported an incidence for posterolat knee tears of 9.1% among all acute knee injuries with hemathrosis (331 patients) [2]. Mechanisms for these traumas are untypical and consist of „sudden external rotation of the tibia with a partial flexed weight-bearing knee“ [3]. MRI has been described as reliable method for detection of lesions of this complex [1]. Lesions of muscle belly and tendon lesions of popliteus can be easily differentiated on MRI [4].
Isolated lesions of the politeus muscle are rare findings. A complete rupture of popliteus leads to a posterolateral instability of the knee while minor lesions induce pain and reduce smoothness [5].
Treatment of minor lesions without instability has been recommended as conservative. Surgery is beneficial for major lesions when origin and/ or advance of the popliteus muscle are dislocated [6]. Guha AR et al. gave a review of the literature in 2003 concerning surgical and conservative management of popliteus tendon tears. Based on the given data they concluded that if a knee is stable though a politeus tear is obvious surgery may not be superior to conservative treatment and proposed a clinical long term follow up to prove efficacy of conservative treatment [5].
Differential Diagnosis List
Final Diagnosis
Myotendinous tear popliteus muscle with extensive edema.
Liscense
Figures
Plain T1TSE cor.

Tirm cor.

Plain T2TSE tra at femoral condyle level

Plain T2TSE tra at level of myotendinous junction of popliteus.

Plain T2*medic sag.
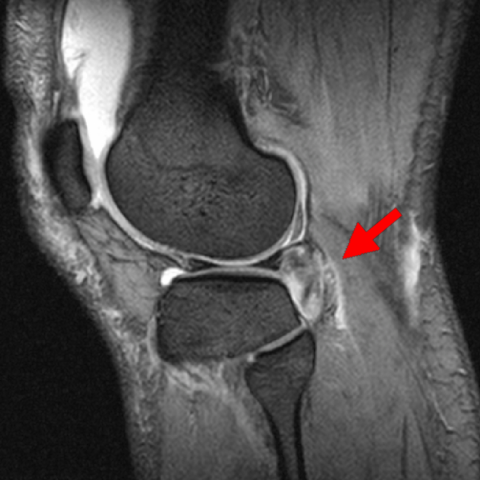
Plain T2TSE sag.

Medical Imaging Analysis Report
1. Radiological Findings
Based on the MRI images of this patient (47 years old, male, left knee injury):
- Abnormal signals are observed in the posterolateral structures of the knee joint, primarily involving the lateral head of the gastrocnemius and the popliteus region. There are signal changes in the popliteus tendon and muscle belly, suggesting a possible partial tear or traction injury.
- The posterior cruciate ligament (PCL) appears incomplete or shows discontinuity, consistent with a post-traumatic tear.
- A portion of edematous signal is noted around the posterolateral popliteal fossa, with soft tissue effusion or a small amount of fluid, indicating soft tissue injury and localized inflammatory changes.
- The lateral collateral ligament (LCL) shows no clear signs of rupture, but mild edema is seen along its course, possibly indicating minor traction or attachment site injury involving related structures.
2. Possible Diagnoses
Based on the imaging findings and clinical history, the primary considerations include:
- Popliteus Tendon or Muscle Belly Tear: The popliteus is an important stabilizing structure on the posterolateral side. Traction or twisting injuries can cause partial or complete tears, commonly leading to posterolateral knee pain and instability.
- Posterior Cruciate Ligament (PCL) Injury: The MRI shows signal interruption or fiber defects in the PCL, which is one of the most significant ligamentous injuries in this case.
- Posterolateral Corner (PLC) Syndrome: Often associated with PCL or other ligament (e.g., LCL) injuries. It is necessary to rule out concurrent damage to the lateral meniscus, ligaments, and other structures.
The above diagnoses may coexist or occur in parallel and require correlation with clinical examination (e.g., external rotation stress test, posterior drawer test) and patient history for comprehensive assessment.
3. Final Diagnosis
Considering the patient’s age, history of trauma (fall with a twist injury to the left knee), and MRI findings, the most likely diagnosis is:
Popliteus tendon and muscle belly injury (partial popliteus tear) combined with posterior cruciate ligament (PCL) tear and mild posterolateral corner damage.
If further confirmation of popliteus tendon tear or the extent of ligament tear is needed, stress MRI of the knee or arthroscopic evaluation may be considered.
4. Treatment Approach and Rehabilitation Plan
1. Treatment Strategies
- Conservative Management: For cases with stable posterolateral corner, partial popliteus tear, and relatively good overall knee stability, conservative treatment with immobilization, bracing, swelling control, pain relief, and gradual muscle strengthening may be considered.
- Surgical Intervention: When there is a significant PCL tear leading to marked instability, or a notable displaced tear of the popliteus tendon, arthroscopic or mini-open repair/reconstruction may be indicated to correct posterolateral instability.
2. Rehabilitation/Exercise Prescription Recommendations
Rehabilitation should be carried out step by step according to the severity of injury and individual circumstances, following FITT-VP principles:
- Phase Goals:
- Acute Phase (1-2 weeks): Focus on reducing swelling and pain, and protecting the injured knee. Braces or knee supports may be used to limit excessive flexion and extension.
- Recovery Phase (2-6 weeks): Gradually restore passive and active range of motion of the knee. Exercises such as straight leg raises and isometric quadriceps contractions can be performed.
- Consolidation Phase (6-12 weeks): Begin partial weight-bearing and increase range of motion under brace protection. Incorporate low-impact functional training, such as stationary cycling or slow walking on flat ground.
- Strengthening Phase (after 3 months): Depending on knee stability, introduce limited-range squats, balance training, resistance band exercises, etc., gradually returning to normal daily or sporting activities.
- Frequency (F): 3-5 times per week, adjusted according to patient tolerance.
- Intensity (I): Start with low intensity, closely monitoring pain and swelling. Gradually increase resistance and range of motion.
- Time (T): 20-30 minutes per session, progressively extending to 30-45 minutes depending on patient tolerance.
- Type (T): Emphasize joint stability exercises and low-impact aerobics (e.g., cycling, elliptical). Later stages may include resistance and proprioception training.
- Progression (P): Advance in stages based on relief of symptoms, restored range of motion, and improvements in muscle strength and joint stability.
Throughout rehabilitation, closely monitor for pain, swelling, or instability. Reduce training load and seek follow-up evaluations if necessary to ensure safety and effectiveness.
Disclaimer: This report is a reference-based analysis using currently available imaging and patient history. It does not substitute for an in-person consultation or professional medical advice. Specific diagnosis and treatment still require clinical assessment and further investigations.
Human Doctor Final Diagnosis
Myotendinous tear popliteus muscle with extensive edema.