Acetabular fracture



Clinical History
Our patient sustained an injury to his right groin. Although his plain radiographs of the pelvis and hip did not reveal any obvious fractures, clinically there was a suspicion of a fracture. He underwent a Multiplanar CT scan, which helped in diagnosing and characterising the acetabular fracture.
Imaging Findings
A 32-year-old male patient who was involved in a road traffic accident was brought to the emergency department. He was the (lap seat belt) back seat passenger when the car had a frontal collision with another car. He sustained a minor head injury and was complaining about pain in the right groin region and over the right iliac crest. Plain radiographs of the pelvis (AP) and right hip (lateral) did not show any obvious fractures.
The patient however was unable to bear weight and had persistent pain in the groin while movement of his hip joint. He underwent a CT scan of the pelvis, which showed a minimally displaced fracture affecting the posterior column of the right acetabulum. He was treated conservatively and had further radiographs including the AP and Judet (oblique) views, which did not show any further displacement of the fracture fragments. He was subsequently discharged for an outpatient follow up.
Discussion
For the purpose of classification of fracture patterns, the acetabulum is divided into an anterior and posterior column. The anterior column comprises the anterior border of the iliac wing, the entire pelvic brim, the anterior wall and the superior pubic ramus. The posterior column comprises the greater and lower sciatic notches, the ischial tuberosity, the posterior wall, and the entire retroacetabular surface.
According to Judet and Letournel classification [1] and column theory, acetabular fractures are classified into simple and complex patterns.
The 5 simple patterns are the following: (account for 20% of acetabular fractures)
1. Posterior wall fractures - posterior wall fractures always involve posterior articular surfaces, often accompanied by a portion of the retroacetabular surface and sometimes the entire surface. The ilioischial line remains intact.
2. Posterior column fractures - bony strut running from PSIS to inferior pubic ramus, and includes the posterior wall. It involves not only the posterior articular surfaces, but also the ilioischial line.
3. Anterior wall fractures.
4. Anterior column fractures - bony strut running from ASIS to superior pubic ramus, and includes anterior wall. The iliopectineal line is involved.
5. Transverse acetabular fractures - involve both anterior and posterior acetabulum: dividing the innominate bone into superior segment containing acetabular roof and intact ilium, and inferior segment consisting of single ischiopubic fragment.
The 5 complex patterns are combinations of the simple patterns: (account for 80% of acetabular fractures)
1. Posterior column with a posterior wall fracture
2. Transverse with a posterior wall fracture
3. T-type fracture - combines a transverse component and vertical component that separates the lower ischiopubic segment into the anterior and posterior columns.
4. Anterior column with a posterior hemitransverse fracture
5. Both-column fracture - all segments of the articular surface are detached from the ilium.
Acetabular fractures must be classified before an appropriate surgical approach can be chosen. Because the Letournel scheme is an anatomic classification, acetabular fracture classification easily follows the radiographic assessment. Such assessment must include AP and Judet views (internal (obturator) oblique and external (iliac) oblique views). CT scans with coronal and sagittal reconstruction are useful in defining the morphologic characteristics of acetabular disruption [2].
Some studies [3] have revealed that MR imaging of acetabular fractures can be used to detect subclinical injury of the sciatic nerve and occult injuries of the femoral head not readily apparent on CT scans. However, intraarticular fragments may be obscured.
Differential Diagnosis List
Final Diagnosis
Displaced fracture affecting the posterior column of the right acetabulum
Liscense
Figures
Plain radiographs

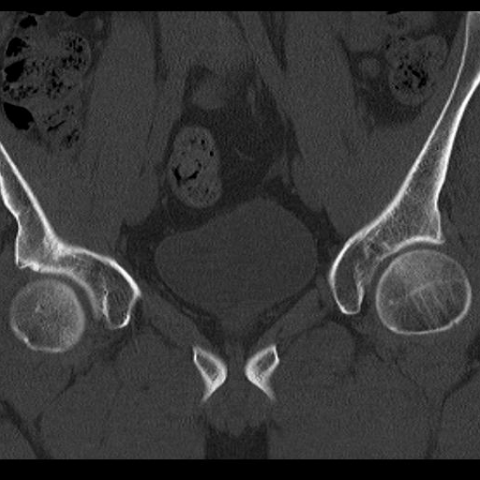
CT axial images




CT coronal images



Follow up Radiographs



1. Imaging Findings
Based on the pelvic and hip X-rays and multi-planar CT scans provided by the patient, a subtle discontinuity in the right acetabular bone can be observed. It is not prominently visible on the plain films, but on CT (axial, coronal, and sagittal reconstructions), the fracture line is more clearly seen, mainly involving the posterior column of the right acetabulum. There is no obvious large swelling or hematoma in the surrounding soft tissue, but a slight increase in soft tissue density suggests a certain degree of soft tissue injury or edema following the trauma. The hip joint space is generally preserved, with no clear signs of dislocation or severe displacement of the hip joint.
2. Potential Diagnoses
Considering the patient’s trauma history and imaging findings, the following possibilities are proposed:
- Posterior Column Fracture: CT shows a fracture line in the posterior column region and possibly involving part of the posterior wall, consistent with one of the simple fracture types (posterior column) according to the Judet and Letournel classification.
- Posterior Wall Fracture: If there is only bony disruption on the posterior articular rim with the ilioischial line remaining intact, a posterior wall fracture should be considered. However, in this case, CT shows the fracture extending into the posterior column, making this possibility slightly lower.
- T-type Fracture: If there was a transverse component plus a longitudinal fracture line separating the ischiopubic ramus, a T-type fracture would be considered. Currently, only a main fracture line in the posterior column is observed, without clear signs of a complete transverse fracture or involvement of both columns.
Based on the available imaging, a posterior column fracture is most suspicious, but comprehensive surgical exploration, clinical examination, and additional imaging should be considered for final confirmation.
3. Final Diagnosis
Taking into account the patient’s age (32 years), trauma mechanism (right inguinal contusion), clinical findings (possible right hip pain and restricted motion), and multi-planar CT findings, the most likely diagnosis is Right Acetabular Posterior Column Fracture (categorized as a simple fracture type under the Judet and Letournel classification).
Should clinical instability or additional imaging findings arise, further evaluation (such as more detailed CT reconstruction or intraoperative exploration) is warranted to rule out a more complex fracture pattern.
4. Treatment Plan and Rehabilitation
Management of a posterior column fracture depends on the degree of displacement, stability, integrity of the joint surface, and the patient’s overall condition (including other pelvic or lower limb injuries). The main recommendations are:
- Conservative Treatment: Indicated for minor displacement, no significant collapse of the articular surface, a stable fracture, or in certain patients who are not candidates for surgery. A brace or use of crutches can protect the affected limb and avoid weight-bearing.
- Surgical Treatment: If there is significant displacement (joint incongruity exceeding 2-3 mm), joint instability, or articular cartilage damage, open reduction and internal fixation (ORIF) can be considered to restore hip alignment and stability.
Rehabilitation / Exercise Prescription (FITT-VP Principle)
-
Initial Phase (Early Protection, 1–3 weeks post-op or post-diagnosis):
- Frequency: 1–2 times per day, focusing on isometric muscle exercises of the affected limb (e.g., quadriceps isometric contraction, holding for 5–10 seconds, then relaxing).
- Intensity: Low intensity, avoiding weight-bearing. Primarily perform gentle joint movements and muscle exercises in a supine or seated position.
- Time: 10–15 minutes each session, divided into segments.
- Type: Avoid large hip movements; ankle pumps, slight straight leg raises (not excessive), and gentle passive range-of-motion exercises to prevent muscle atrophy.
- Progression: Gradually increase the range of motion and number of repetitions as pain decreases.
-
Intermediate Phase (Transition to Weight-Bearing, approximately 3–6 weeks):
- Frequency: 3–4 times per week.
- Intensity: Under physician or therapist supervision, gradually transition to partial weight-bearing (using crutches or a walker), and introduce light resistance exercises for lower extremity muscles (e.g., elastic band resistance).
- Time: Progressively increase to 20–30 minutes per session as tolerated, with breaks as needed.
- Type: Incorporate exercises that improve joint flexibility and core stability, such as seated or standing balance training.
- Progression: Increase resistance or frequency according to fracture healing status, taking care to avoid overloading that could cause re-injury.
-
Late Phase (Functional Recovery, 6–12 weeks and beyond):
- Frequency: 3–5 times per week.
- Intensity: Once good bone healing is confirmed, gradually progress to near-normal weight-bearing; introduce moderate resistance training to strengthen peri-hip muscles.
- Time: 30–45 minutes per session, possibly split into segments depending on tolerance.
- Type: Activities such as stationary cycling, elliptical machines, or swimming with low impact, combined with flexibility, coordination, and proprioception training.
- Progression: Gradually return to daily activities and light sports. High-impact exercises like running should be resumed cautiously based on clinical assessment and patient’s recovery.
Throughout the rehabilitation process, closely monitor changes in symptoms, pain, and range of motion, and schedule regular imaging follow-up. In case of significant worsening of pain or functional impairment, seek medical attention promptly.
Disclaimer
This report is based solely on the available imaging and clinical information and does not replace face-to-face consultation or professional medical advice. For any specific treatment measures or surgical plans, please consult a certified physician and make decisions according to the actual clinical situation.
Human Doctor Final Diagnosis
Displaced fracture affecting the posterior column of the right acetabulum