Osteochondritis Dissecans of the knee, stage 3 – MRI findings



Clinical History
An 18 year old patient presented with right knee pain. MRI exam was performed and the findings are presented.
Imaging Findings
An 18 years old patient with a recent history of injury at the medial aspect of the knee during athletics was referred to the Radiology Department by his GP. He also complained of occasional locking and limitation of movement. MRI was performed.
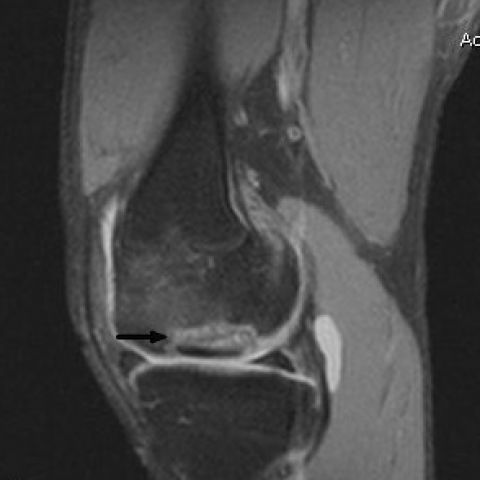
On T1 weighted image (fig 1) there was a hypointense lesion of approximately 1 cm in diameter at the lateral aspect of medial femoral condyle. On T2 and T2 fat suppressed weighted images (Fig 2) the lesion had a zonal morphology and was of low signal intensity with a surrounding rim of high signal intensity. PD sequences (fig 3) demonstrated an osteochondritis lesion of approximately 1 cm with fluid signal intensity between the fragment and the donor site. Additionally, subchondral edema was noted at the surrounding bone tissue (fig 4a,b).
Discussion
In this case, MR imaging demonstrated an osteochondral defect on the lateral aspect of the medial femoral condyle and its partially detachment with fibrous tissue interposition. These features are characteristic of osteochondritis dissecans.
Osteochondritis dissecans (OCD) refers to the acquired fragmentation and possible separation of the articular cartilage and a segment of subchondral bone from the remaining articular surface. Etiology relates to a subchondral fatigue fracture usually as a result of shearing, rotatory or tangentially aligned impaction forces. This may relate to a single traumatic episode or multiple repetitive. Clinically the most common signs are intermittent locking, recurrent effusions, crepitus and persistent pain. The condition usually occurs in younger patients and more commonly in males.
A grading system is used ranging from subchondral contusion with intact articular cartilage (stage 1) to frank separation of an unstable osteochondral fragment (grade 4). The stage-like course of the development of OCD is as follows (fig 5):
Grade 1: Subchondral osseous lesion. The cartilage coverage is macroscopically intact.
Grade 2: Articular cartilage defect without loose body
Grade 3: Partially detached osteochondral fragment.
Grade 4: Loose body formation
In our case the osteochondral fragment was partially detached with fibrous tissue interposition and is classified as osteochondritis dissecans of stage 3.
Plain-film findings are usually negative in the initial stages and the overlying cartilage integrity cannot be assessed. In some patients a subchondral fracture may be seen and in chronic cases there may be subchondral sclerosis. Computed tomography (CT) may or may not demonstrate the subchondral fracture and sclerosis. CT arthrography may demonstrate the chondral defect filled with contrast. MRI is the non-invasive test of choice, as both chondral and subchondral lesions are seen. The associated subchondral fracture or oedema appears hypointense on T1WI and the chondral defect with or without the associated subchondral bone marrow oedema is best demonstrated on FS intermediate WI.
Treatment of osteochondritis dissecans is typically nonoperative for stable lesions and operative for unstable lesions. Unstable lesions can be treated arthroscopically by drilling, which affects bone repair, with subsequent healing. If the central bone fragments are of sufficient size they may be internally fixed with bone pegs or Herbert screws. Outcome depends on a number of factors, including the location and size of the lesion, patient age and treatment. A good clinical outcome is likely when the femoral growth plate is open, when the lesion is small and is stable on MRI. When a cartilage fracture or articular defect is found on MRI, the patient is likely to have a poor outcome.
Differential Diagnosis List
Final Diagnosis
Osteochondritis dissecans of the knee, stage 3
Liscense
Figures
T1WI, sagittal plan

T2WI with fat suppression, sagittal plan

Sagittal PD fat saturated image
Tirm image, coronal plan


Osteochondritis dissecans: schematic drawing of the 4 stages





Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided knee MRI images, the following main features are observed:
- The lesion is located on the lateral side of the medial femoral condyle of the right knee joint (i.e., the outer edge of the medial condyle).
- On T1-weighted images, a local low signal area is visible in the restricted region, indicating a possible subchondral fracture or bony changes.
- On fat-suppressed sequences (e.g., FS T2 or FS PD), subchondral bone marrow edema or bone marrow signal hyperintensity is noted, with a certain degree of reduced clarity at the margins.
- Partial discontinuity of the cartilage surface is seen, suggesting a tear or defect involving the local cartilage and subchondral bone.
- A partially detached osteochondral fragment is visible, showing signs of fibrous tissue infiltration.
In summary, these findings are consistent with signs of a locally unstable osteochondral segment.
II. Potential Diagnosis
Based on the patient’s age, symptomatic presentation (knee pain), and MRI findings showing local osteochondral defects with subchondral bone changes, the following diagnoses or differentials are considered:
- Osteochondritis Dissecans (OCD)
Cause: Common in adolescents, potentially due to repeated microtrauma or a single injury causing excessive stress on the subchondral bone of the femoral articular surface.
Characteristics: MRI may show abnormal subchondral signals, bone marrow edema, and partial or complete separation of an osteochondral fragment. When unstable, significant detachment is observed. This aligns with the patient’s presentation. - Local Cartilage Ulceration or Traumatic Cartilage Injury
Cause: Acute trauma or excessive rotational/shearing forces leading to a localized cartilage defect.
Characteristics: MRI typically shows irregular or abnormal cartilage surface signals, but without significant bony changes, it is less typical than OCD. - Subacute or Chronic Bone Bruise
Cause: Usually caused by knee impact or twisting injuries leading to subchondral edema.
Characteristics: Edema is visible on T2 or fat-suppressed sequences, but there may not be a clear osteochondral fissure or fragment separation.
Considering the imaging characteristics and clinical information, OCD is the primary concern.
III. Final Diagnosis
Combining the patient’s gender, age (18 years old, adolescent—common OCD demographic), clinical symptoms (knee pain), and MRI findings, the diagnosis can be confirmed as:
Osteochondritis Dissecans (OCD) of the lateral side of the medial femoral condyle in the right knee, in a partially detached stage (OCD Stage III).
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Conservative Treatment: Suitable for earlier OCD stages (Stage I or II) with stable lesions or patients whose growth plates have not closed. Approaches may include reducing weight-bearing, using knee braces or supports, and engaging in rehabilitation exercises.
- Surgical Treatment: For this case, with a partially detached osteochondral fragment (Stage III) and signs of instability, surgical intervention is often required. Common procedures include:
- Arthroscopically guided drilling to decompress and promote bone healing.
- If the detached fragment is large and still viable, fixation procedures (e.g., bone screws or Herbert screws) may be performed.
- In severe cases or where fragments are not repairable, cartilage transplantation/repair surgery may be considered.
2. Rehabilitation/Exercise Prescription Recommendations
The goals of rehabilitation are to relieve pain, promote osteochondral healing, and restore joint range of motion and function. A gradual, individualized approach following the FITT-VP principle (Frequency, Intensity, Time, Type, Progression, and Volume) is recommended. The following is a brief example:
- Postoperative or Early Conservative Phase (about 2–4 weeks):
- Frequency: 3–4 times per week, avoiding excessive weight-bearing.
- Intensity: Focus on range of motion exercises with gentle movements, such as seated knee extension and ankle pumps.
- Time: Approximately 20–30 minutes per session, with rest intervals.
- Type: Non-weight-bearing or partial weight-bearing activities (e.g., straight leg raises, isometric contractions) to maintain or improve quadriceps and lower limb muscle strength.
- Mid-Phase Functional Training (approximately 4–8 weeks):
- Frequency: 3–5 times per week.
- Intensity: Light weight-bearing exercises can be introduced cautiously, avoiding movements that produce significant pain.
- Time: Each session can last 30–45 minutes.
- Type: Further improvement of range of motion, using resistance bands or low-resistance machines to train the quadriceps and hamstrings. Stationary cycling or aquatic exercises may be incorporated.
- Late-Phase Return to Activity (after about 8 weeks):
- Frequency: 3–5 times per week, depending on joint stability and pain relief.
- Intensity: Gradually progress to moderate-intensity training, cautiously introducing slow jogging or walking on flat surfaces.
- Time: 40–60 minutes per session, may be extended as tolerated.
- Type: Functional strength and flexibility exercises, including low-impact running and jumping drills (if no significant pain or swelling), supplemented with balance training (e.g., single-leg standing).
If the patient experiences significant pain, joint swelling, or worsening functional impairment during rehabilitation, reduce or pause the exercises and seek medical advice promptly.
3. Special Considerations
- Monitor the patellofemoral and femorotibial joints closely during training, avoiding high-impact repetitive stress on the affected area.
- Supportive devices, such as braces, knee supports, or crutches, may be used to reduce weight-bearing, especially during early rehabilitation.
- If the patient has other joint or soft tissue conditions, adjust the training schedule individually and, when possible, conduct rehabilitation under the guidance of a professional therapist or physician.
Disclaimer
This report is based solely on the available imaging and medical history, serving as a reference analysis. It does not replace an in-person consultation or professional medical advice. If there are any questions or changes in the patient’s condition, please seek timely evaluation at a qualified medical facility.
Human Doctor Final Diagnosis
Osteochondritis dissecans of the knee, stage 3