Not all back pain is created equal



Clinical History
A 74-year-old female was referred from outpatient orthopaedic clinic for an MRI spine after presenting with groin, back and hip pain on mobilisation. Past medical history included osteoarthritis, right total hip replacement and previous hysterectomy.
Imaging Findings
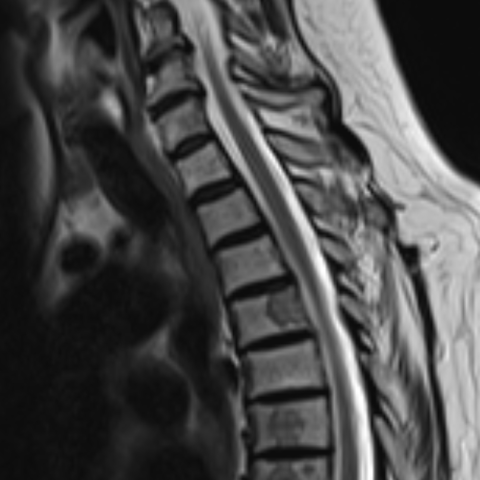
Initial MRI spine showed rounded T1 low signal bone marrow foci throughout the whole spine suspicious for metastatic deposits without cortical breakthrough, cord compression or canal stenosis.
Follow up CT Thorax, Abdomen and Pelvis showed multiple bilateral pulmonary nodules, with a dominant 13mm right upper lobe nodule and ipsilateral mediastinal lymphadenopathy, measuring up to 15mm in the right lower paratracheal station together with smaller hilar lymph nodes. Multiple sclerotic lesions were confirmed throughout the axial skeleton. There was no intra-abdominal disease.
CT-guided percutaneous biopsy of an L2 sclerotic lesion gave the diagnosis.
Discussion
Sarcoidosis is well known as the ‘great mimic’ and the path to diagnosis is not always a straightforward one. Between one-third and one-quarter of people with sarcoidosis have some form of musculoskeletal involvement, most commonly presenting as small joint arthropathy [1]. Bone involvement is thought to be less common, occurring in an estimated average of 5% of patients [2]. It is postulated however, that the prevalence of osseous sarcoid is much higher owing to the fact that it is most often asymptomatic [3, 4] and remains undetected unless patients undergo advanced imaging. In this case osseous sarcoid was the primary cause for presentation, which is a rare occurrence given its tendency to develop later in the disease, when other systemic manifestations are more likely to already be present [3, 4, 5].
The imaging appearances of bone involvement are many with no specific pattern to rely upon and these often emulate that of a neoplastic process. Bone lesions can show increased uptake on technetium bone scan. On CT imaging these may be destructive, sclerotic or even undetectable [6]. Lesions have variable marrow signal changes on MRI[2][5], with no reliable discriminators to accurately differentiate sarcoidosis from malignancy [6]. Therefore, histological evidence is pivotal in making a diagnosis [7, 8]. Pursuing and ruling out more common pathologies, such as metastatic malignancy, should usually take precedence especially if there is not already an established diagnosis of sarcoidosis.
In this case, the patient’s presenting complaint was groin, hip and back pain. Following the initial MRI spine and subsequent CT, the patient was discussed in both Cancer of Unknown Primary and Lung cancer Multidisciplinary Team Meetings (MDT). The main differential diagnoses were that of metastatic cancer or lymphoma. An Endobronchial Ultrasound (EBUS) guided biopsy of a 4R lymph node was inadequate and the right upper lobe nodule was deemed unsuitable for biopsy. A lesion in the left upper portion of L2 was the next best option for tissue diagnosis. Histology revealed necrotizing granulomata in keeping with sarcoidosis and the patient was commenced on corticosteroid therapy.
At 6 months follow up, the patient was still on a tapering course of Prednisolone, and her symptoms did not mandate any dedicated follow up of her spinal lesions. These are, however, still visible on the only subsequent imaging performed at the time, a High Resolution Computed Tomography (HRCT) of her thorax, and had not yet regressed.
All patient data have been completely anonymised throughout the entire manuscript and related files.
Differential Diagnosis List
Final Diagnosis
Sarcoidosis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures










Radiological Findings
In this case, MRI of the lumbar and thoracic spine shows multiple abnormal signals in the vertebral bodies. The lesions appear as patchy or spot-like low-, high-, or mixed signals on different sequences. Overall, the bone cortex remains relatively intact, with no prominent signs of collapse. CT scans reveal pulmonary nodules and enlarged lymph nodes. In the lumbar spine (particularly the L2 vertebra), there is an abnormal density area with indistinct borders; in some regions, the bone is slightly osteoporotic or sclerotic. These findings have no clear specificity and can be easily confused with metastatic tumors or lymphoma. Overall, imaging suggests multiple lesions in the spine, and further differentiation with pathology is needed.
Potential Diagnoses
- Metastatic Tumor: The patient is older, and multiple bone lesions are commonly seen in metastatic cancer. Radiologically, they often present as multiple, irregular lytic or sclerotic lesions, especially under circumstances where there is a history of malignancy or high-risk factors.
- Lymphoma: Lymphomatous involvement of bone can also cause multiple bone lesions, accompanied by thoracic, abdominal, or generalized lymph node enlargement. However, in this case, EBUS-guided lymph node sampling did not indicate lymphoma.
- Other Granulomatous Diseases: Such as tuberculous lesions or fungal infections, which typically exhibit more pronounced vertebral destruction, paravertebral abscesses, or other signs of infection.
- Sarcoidosis: Sarcoidosis can involve bone, presenting as multiple or localized lesions, often accompanied by pulmonary changes or lymph node enlargement. Imaging findings may resemble malignancy, and pathological confirmation is required.
Final Diagnosis
Based on the radiological findings, histopathological examination of vertebral biopsy showing caseating granulomas, as well as the clinical presentation of lung nodules and lymph node enlargement, the most likely diagnosis is:
Sarcoidosis involving the spinal skeleton.
Treatment Plan and Rehabilitation Program
The patient has already started corticosteroid therapy. For sarcoidosis with significant skeletal involvement, the standard treatment plan includes:
- Medication: Corticosteroids (e.g., prednisolone) as first-line therapy, which can be combined with immunosuppressants (e.g., methotrexate) as needed.
- Symptomatic and Supportive Care: If bone lesions lead to significant pain or functional impairment, pain relievers, bone-protective agents (e.g., bisphosphonates), and adequate calcium and vitamin D supplementation may be required.
- Follow-up and Re-examination: Regular imaging follow-up (X-ray, MRI, or CT) and pulmonary function tests can help assess treatment effectiveness and detect any new lesions.
From a rehabilitation and exercise perspective, it is necessary to account for the patient's age, bone quality, and cardiopulmonary function to develop a safe and gradual regimen. Following the FITT-VP principle:
- Exercise Type (Type): Begin with low-intensity range-of-motion exercises and light resistance training, such as seated or supine leg raises and mild back exercises, while avoiding high-impact loading.
- Frequency (Frequency): Start with 2-3 sessions per week, gradually increasing to 3-5 sessions, according to fatigue level and pain status.
- Intensity (Intensity): In the early stages, keep it at a low intensity that does not cause significant pain. This can be monitored through perceived exertion (RPE around 3-4) or heart rate.
- Duration (Time): Each session can begin at 10-15 minutes and gradually increase to 30 minutes. If tolerated, it may extend to 30-45 minutes in later stages.
- Training Volume and Progression (Volume & Progression): As tolerance improves, slightly increase session duration or resistance. Reassess the exercise volume every 1-2 weeks to ensure safety.
Patients with fragile bones should avoid excessive weight-bearing and high-impact exercises. Individuals with a history of hip replacement should be careful to avoid excessive adduction or internal rotation. Adhere to a gradual, individualized exercise approach.
Disclaimer: This report provides only a reference-based analysis based on the available imaging and data, and is not a substitute for in-person consultation or professional medical advice. Specific diagnosis and treatment plans should be determined in conjunction with clinical circumstances and relevant specialist discussions.
Human Doctor Final Diagnosis
Sarcoidosis