Cubital tunnel syndrome due to anconeus epitrochlearis muscle



Clinical History
A 21 year old male with intermittent pain in the medial side of the left elbow and hand paresthesia, while playing tennis.
Imaging Findings
A 21 year old male presented with intermittent pain in the medial side of the left elbow and hand paresthesia in the ulnar nerve distribution of 3 months duration, while playing tennis. There was neither history of elbow trauma nor any sign of ulnar nerve subluxation or dislocation during elbow flexion and extension.
An MR examination was performed using the routine protocol at our institution for elbow pain that encompasses T1-weighted fast spin echo images in all 3 planes, fat-satured (FatSat) proton density-weighted sequences in axial and coronal planes and a gradient echo T2*-weighted sequence in the sagittal plane.
A surface coil and a 1.0 open MR scanner were used to obtain all images.
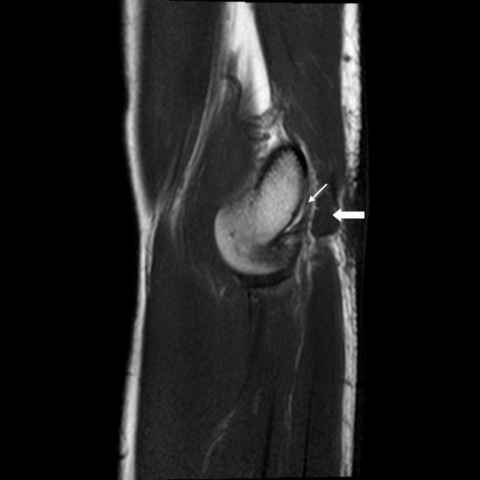
An accessory muscle - anconeus epitrochlearis - was demonstrated on the postero-medial aspect of the elbow. The ulnar nerve was swollen and oedematous in the cubital tunnel, with oedema of the perineural fat, findings consistent with ulnar neuropathy secondary to intermittent compression of the nerve by the anconeus epitrochlearis muscle.
Discussion
Second only to carpal tunnel syndrome, cubital tunnel syndrome is the most frequent compressive neuropathy of the upper limb in young adults. Ulnar nerve compression in the cubital tunnel can have different causes, including space occupying lesions in the cubital tunnel (synovial cyst, synovial tumour or osteophytes), trauma (elbow fracture or dislocation, activity related repetitive microtrauma), cubitus varus or valgus, overuse syndrome, tourniquet paralysis, congenital anomalies (accessory muscle), local swelling due to metabolic or endocrine disease (pregnancy, acromegaly, thyroid disease, amyloidosis, pseudotumoral calcinosis), and systemic diseases (rheumatoid arthritis, systemic erythematosus lupus, sclerodermia) [1].
The anconeus epitrochlearis muscle is a supernumerary muscle that takes the same course as the cubital tunnel retinaculum in the postero-medial aspect of the elbow, running superficial to the ulnar nerve from the inferior surface of the medial epicondyle to the medial cortex of the olecranon. As the elbow moves from extension to flexion, the cross-sectional area of the cubital tunnel decreases and the anconeus epitrochlearis muscle may compress de ulnar nerve in the cubital tunnel [2]. Besides, the anconeus epitrochlearis muscle may compress the nerve as it contracts and its thickness increases. The cubital tunnel retinaculum is thought to be the remnant of the anconeus epitrochlearis. The reported prevalence of the anconeus epitrochlearis from cadaveric studies is 11%. The anconeus epitrochlearis can be identified at US or, more accurately, at MR imaging [3].
In our patient, the anconeus epitrochlearis muscle was best seen on axial images, where the relationship between the ulnar nerve and adjacent structures could be better demonstrated (Fig 1). We think that in our case the anconeus epitrocleares muscle was the cause of the patient's ulnar neuropathy.
Initial treatment for acute and subacute ulnar neuropathy at the elbow is nonsurgical. Rest and avoidance of pressure on the nerve may suffice. If symptoms persist, activity modification, splint immobilization, NSAIDS, infiltrations and physical therapy can be tried. For chronic neuropathy associated with muscle weakness, or for neuropathy that does not respond to conservative measures, surgery is usually necessary - incision and splitting of the accessory muscle is usually enough to obtain ulnar nerve decompression and resolution of the symptoms [4].
Our patient used to be a heavy tennis player and complained mainly of exercise triggered elbow pain without significant hand paresthesias. For treatment he stopped playing tennis and underwent physical therapy and is doing better.
Differential Diagnosis List
Final Diagnosis
Cubital tunnel syndrome due to anconeus epitrochlearis muscle
Liscense
Figures
Axial MR images



Coronal MR images



Sagittal MR images

Medical Imaging Analysis Report
1. Imaging Findings
This 21-year-old male patient reports intermittent medial elbow pain during tennis activity, accompanied by sensory abnormalities in the hand. Based on the provided MRI images, the following findings are noted:
- On the posteromedial side of the elbow joint, there is a muscle attached to the lower margin of the medial epicondyle and extending to the medial cortex of the olecranon. Its course is above the ulnar nerve and closely related to it, consistent with the imaging appearance of the anconeus epitrochlearis muscle.
- No obvious fracture, significant osteoblastic or osteolytic lesions are observed, and there is no significant effusion in the joint space.
- When the elbow is flexed, this accessory muscle thickens and may potentially compress the ulnar nerve, suggesting a possible “cubital tunnel syndrome.”
2. Potential Diagnoses
Based on the patient’s clinical symptoms (medial elbow pain triggered by activity and hand sensory abnormalities) and the abnormal muscular structure seen on imaging, the potential diagnoses include:
- Cubital Tunnel Syndrome:
- Caused by hypertrophy or abnormal course of the anconeus epitrochlearis muscle (sometimes referred to as a supporting band over the cubital tunnel), or other space-occupying factors leading to ulnar nerve compression within the cubital tunnel.
- The pathological mechanism involves chronic mechanical compression or traction of the ulnar nerve.
- Other Soft Tissue Lesions Involving Ulnar Nerve Irritation (e.g., fibrosis, synovial cysts, etc.):
- In this case, no clear cystic or significant soft tissue mass is seen on imaging, but it remains a differential consideration.
3. Final Diagnosis
Taking into account the patient’s young age, the activity-induced nature of the symptoms, and the anatomical variation of the anconeus epitrochlearis muscle shown on imaging with potential compression of the ulnar nerve, the most likely diagnosis is:
Cubital tunnel syndrome caused by the anconeus epitrochlearis muscle.
If diagnostic uncertainty remains, further electromyography or nerve conduction studies are recommended to confirm the site and degree of ulnar nerve compression.
4. Treatment Plan and Rehabilitation
Based on the current situation, where symptoms primarily worsen during sports and hand sensory changes are not severe, conservative measures are initially advised. If symptoms persist or worsen, surgical decompression may be considered.
1. Conservative Treatment
- Rest and Avoidance of Compression: Reduce or temporarily stop tennis activities or other repetitive elbow flexion-extension movements that provoke symptoms. Avoid external pressure or prolonged support on the medial elbow.
- Brace Application: A brace can be used at night or during extended periods when the elbow is flexed, maintaining a slight extension to reduce traction and compression on the ulnar nerve.
- Medication and Physical Therapy: Nonsteroidal anti-inflammatory drugs (NSAIDs) may help alleviate local inflammation and pain. Physical therapy modalities (e.g., heat application, ultrasound therapy) can improve local blood flow.
2. Surgical Treatment
If the patient experiences persistent or worsening sensory disturbances, muscle weakness, unbearable pain, or if conservative treatment fails, surgical intervention should be considered:
- Surgical exploration and management of the anconeus epitrochlearis muscle (e.g., partial resection or release) to relieve ulnar nerve compression.
- Postoperative rehabilitation is essential to restore joint function and nerve conduction.
3. Rehabilitation and Exercise Prescription
During both conservative management and postoperative recovery, an individualized exercise plan can be designed using the FITT-VP principles (Frequency, Intensity, Time, Type, Volume, Progression):
- Frequency: Early stages typically involve 1–2 sessions per day targeting elbow flexibility, gradually increasing to 2–3 sessions/day.
- Intensity: Begin with gentle stretching or isometric muscle exercises within the pain tolerance range.
- Time: Each session may last about 10–15 minutes initially, with possible gradual extension as tolerance and muscle strength improve.
- Type:
- Choose mild range-of-motion exercises (e.g., active elbow flexion-extension) and light isometric contractions of the forearm muscles.
- After surgery or when symptoms improve, progressively introduce resistance exercises (e.g., using elastic bands) to strengthen surrounding muscle groups.
- Volume: Increase gradually according to patient tolerance. Initially, 2–3 sets of 10–12 repetitions per session are recommended.
- Progression: As symptoms lessen and strength improves, gradually increase resistance or the range of flexion-extension. However, avoid excessive loading at once.
Throughout the rehabilitation process, closely monitor symptom changes. If pain or sensory disturbances worsen, re-evaluate and adjust the plan accordingly.
Disclaimer
This analysis report is based solely on the clinical and imaging data currently available and is provided for reference purposes. It is not a substitute for in-person consultation or professional medical advice. For diagnosis and treatment decisions, a comprehensive evaluation of the patient’s condition and additional medical test results by a qualified physician is essential.
Human Doctor Final Diagnosis
Cubital tunnel syndrome due to anconeus epitrochlearis muscle