Infantile Cortical Hyperostosis



Clinical History
A 4 months old male child was brought to the hospital with a history of fever, irritability and excessive crying. Mild swelling and tenderness was noted over the lower ends of both forearms and both sides of root of the neck. Investigations were done. X ray features were diagnostic.
Imaging Findings
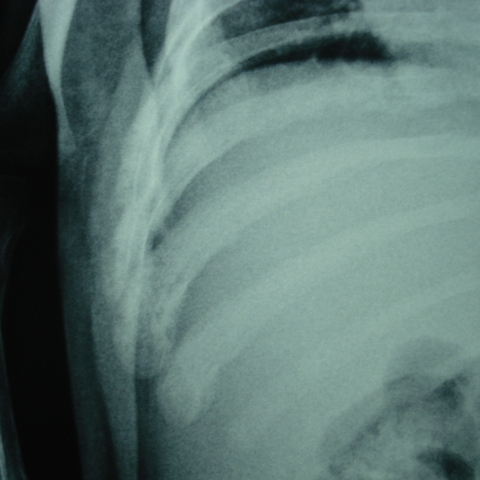
A 4 months old male child was brought to the paediatric department by his parents with a history of fever, irritability and excessive crying for two weeks. There was no history of trauma. There were no further relevant details in the past medical history. On clinical examination, there was a palpable swelling on lower end of both forearms which were tender. Palpable hardness with tenderness also elicited over clavicular regions. However, overlying skin appeared relatively normal. No palpable regional lymphadenopathy detected. Serologic investigations for viral and bacterial infections were negative. Sedimentation rate and alkaline phosphatase were high. The clinical impression was of an inflammatory condition due to systemic cause. The patient was subjected to X ray of chest (Fig ) including both hands which revealed cortical hyperostosis involving diametaphyseal regions of both radiuses (Fig 2,3) and diaphyses of both clavicles (Fig 4,5). Careful examination of chest X ray revealed similar changes of lower ribs (Fig 6) and mandibles (Fig 7,8) though to a lower extent. The X ray findings were suggestive of infantile cortical hyperostosis or Caffey’s disease. Palliative treatment was given and the symptoms subsided after 6 weeks.
Discussion
Infantile cortical hyperostosis or Caffey’s disease is a rare disorder affecting the skeleton and some of its contiguous fasciae and muscles, mainly involving children below 1 year of age group. The cause is unknown and pathogenesis is obscure. Caffey and Silverman first reported this disease as a distinct entity in 1945. Cases are seen in all manner of circumstances – in cities and rural communities, in poverty and luxury, in all climates and in all races with no sex preference. There is a striking age limitation with majority cases appear before 5th-7th month of life. Average age at onset is 9 weeks. The disease is self limiting and symptoms lasting from 2-3 weeks to 2-3 months.
There are 3 main manifestations common to all patients: hyperirritability, swelling of the soft tissues and cortical thickenings of the underlying bones. The soft tissue swelling appears suddenly at the onset and present as painful wooden hardness during the active phase of the disease. They are almost always deeply situated and do not extend up to the subcutaneous tissue or are not overly warm or discoloured. Swelling subsided long before hyperostosis resolves.
The radiographic features are the sine qua non for diagnosis. Hyperostosis develops in contact with external cortical surface, expands and then remodel by resorption externally or expansion from internal aspects of bone. Cortical hyperostosis has been demonstrated in all the tubular bones of the skeleton except the phalanges. Vertebral bodies are spared. Mandible, clavicles and ulna are most commonly affected bones.
Complications depend upon the site of involvement. Pseudoparalysis, pleural effusion and dysphagia are reported. Most common laboratory findings are raised erythrocyte sedimentation rate and alkaline phosphatase. Thrombocytosis is more common than thrombocytopenia. Anemia is common. Differential diagnosis includes injury, vitamin A toxicity, syphilis, scurvy, osteomyelitis, parotitis and malignancy. The majority of these conditions can be ruled out by age group, demonstrating mandibular involvement, and observing triad of irritability, swelling and osseous lesions etc.
As it is a self limiting condition, palliative treatment is the one which is generally given. Long lasting morbidity or mortality is rare in this condition.
Differential Diagnosis List
Final Diagnosis
Infantile Cortical Hyperostosis or Caffey's Disease.
Liscense
Figures
Chest X ray

AP view of left forearm

AP view of right forearm

Chest xray (AP View)

AP view of left clavicle

X ray of right lower chest
X ray of mandible( right lateral view)

X ray of mandible ( left lateral view)

Radiological Findings
Based on the provided X-ray images, the following key features are observed:
- Marked thickening of the cortices of the radius and ulna in both forearms, showing relatively uniform cortical hypertrophy;
- Similar cortical hyperostosis observed in the clavicle region;
- Cortical thickening or abnormalities are also noted in the ribs and jawbone;
- The aforementioned thickening is not caused by local fractures, and no clear fracture lines or bone defects are evident. The range of soft tissue swelling corresponds to the areas of cortical thickening.
Regarding soft tissues, there is local swelling but no obvious subcutaneous air, exudate, or abscess formation. Overall, there are no signs of bone marrow cavity invasion or bone destruction. The radiological findings correlate with the regions of swelling observed in both forearms and the base of the neck in the patient.
Potential Diagnoses
Considering the patient's clinical presentation (fever, irritability, local swelling, and pain) along with the radiological features (bone cortical thickening, soft tissue swelling), the following differential diagnoses should be considered:
- Infantile Cortical Hyperostosis (Caffey Disease)
Characteristics: A classic triad of irritability, soft tissue swelling, and bone cortical hyperostosis. Commonly affects the mandible, clavicle, and ulna. Typically presents at a few weeks to months of age and is generally self-limiting. - Osteomyelitis / Infectious Lesions
Characteristics: May present with localized pain, fever, and abnormal X-ray findings, often accompanied by bone destruction, periosteal reaction, or abscess formation. Clinical and laboratory inflammatory markers are usually more pronounced. - Vitamin Deficiency (e.g., Scurvy)
Characteristics: May exhibit changes at the metaphyses, soft tissue hemorrhage, or gum bleeding. Typically, findings such as the “white line” or “corner sign” are present, which do not fully align with the cortical thickening visible in this case. - Traumatic Bone Changes
Characteristics: An obvious history of trauma is usually present, and fracture lines or localized periosteal reactions are often visible. This does not adequately explain the bilateral, symmetrical thickening observed in this case. - Tumors or Tumor-like Lesions
Characteristics: Malignant small round cell tumors or osteosarcomas typically show focal bone destruction or irregular new bone formation. Additionally, the patient’s age, symptoms, and disease progression do not match these conditions.
Final Diagnosis
After comprehensive analysis: The patient, approximately 4 months old, falls within the typical age range for Caffey Disease (Infantile Cortical Hyperostosis). Clinical symptoms include fever, irritability, swelling of the forearms and base of the neck, and no significant purulent signs. Radiological findings demonstrate symmetrical cortical thickening and new bone formation in both the radius and ulna, as well as in the clavicle, consistent with hallmark presentations of Caffey Disease. Given the disease’s self-limiting nature and corresponding laboratory findings (elevated serum alkaline phosphatase, elevated erythrocyte sedimentation rate, etc.), the most likely final diagnosis is:
Infantile Cortical Hyperostosis (Caffey Disease).
Treatment Plan and Rehabilitation
As Caffey Disease is self-limiting, most pediatric patients recover within weeks to months. Treatment is primarily conservative and symptom-relieving, with vigilant monitoring of disease progression. For pain and fever, recommended approaches include:
- Medication Therapy:
- Use appropriate doses of antipyretic and analgesic medications (such as acetaminophen or ibuprofen) to reduce pain and discomfort;
- In the absence of severe infection, antibiotics are generally not necessary;
- If severe pain affects feeding or sleep, short-term analgesics under medical supervision may be used.
- Monitoring and Follow-up:
- Regularly monitor the patient’s body temperature and inflammatory markers, such as complete blood count, erythrocyte sedimentation rate, and alkaline phosphatase levels;
- Follow-up X-rays to track the progression or remodeling of the cortical thickening.
In terms of rehabilitation, although this condition typically has minimal long-term impact on bone morphology, it is important to reduce strain on affected areas during the acute phase to avoid aggravating pain or periosteal irritation.
-
Early Recovery Phase (Active Disease Stage)
Recommend minimizing excessive activity of the affected forearms and other involved areas. Gentle passive stretching and movement can be performed with caregiver support to relieve muscle tension. Conduct these activities 2–3 times per day, each lasting 1–3 minutes, with gentle, slow motions. -
Intermediate Consolidation Phase (Symptom Relief Stage)
Gradually increase the range of motion in the arms and upper limbs. Include natural movements during routine care activities such as holding, feeding, or playing. Avoid sudden or forceful pulling or twisting. Gentle passive joint movements and soft-toy grasping exercises can be performed 2–3 times per day, for 3–5 minutes each. -
Late Functional Recovery (Complete Resorption Stage)
When symptoms have substantially improved, allow the patient to engage in normal developmental activities such as rolling over and crawling. At this stage, exercise sessions can be extended to 2–3 times per day, each for 5–10 minutes, adjusting according to the patient’s tolerance.
Exercise or rehabilitation plans should follow a gradual, stepwise approach, taking the child’s response and developmental level into full consideration. If the child experiences marked pain, pronounced irritability, or a resurgence of fever, a medical evaluation is advised, and related exercises should be suspended if necessary.
Disclaimer:
This report, based on the provided clinical and imaging information, is intended for reference only and does not replace an in-person consultation or professional medical advice. If you have any questions or notice any change in condition, please seek guidance from a qualified healthcare professional or specialist promptly.
Human Doctor Final Diagnosis
Infantile Cortical Hyperostosis or Caffey's Disease.